

Functional, cognitive and physical outcomes 3 years after minor lacunar or cortical ischaemic stroke
- PMID: 30554134
- PMCID: PMC6581154
- DOI: 10.1136/jnnp-2018-319134
Functional, cognitive and physical outcomes 3 years after minor lacunar or cortical ischaemic stroke
Abstract
Objective: Many studies examining stroke outcomes focus on more severe strokes or have short follow-up periods, so the long-term outcomes post-minor ischaemic stroke are unclear.
Methods: We recruited participants from inpatient and outpatient services with a lacunar or minor cortical ischaemic stroke (National Institutes of Health Stroke Scale score <8) and assessed current and premorbid cognitive functioning (Addenbrooke's Cognitive Examination-Revised (ACE-R), National Adult Reading Test (NART)), physical functioning (Timed Get Up and Go (TUG), 9-Hole Peg Test (9HPT)), dependency (modified Rankin Scale (mRS)), depression (Beck's Depression Inventory) in-person and remotely (Stroke Impact Scale).
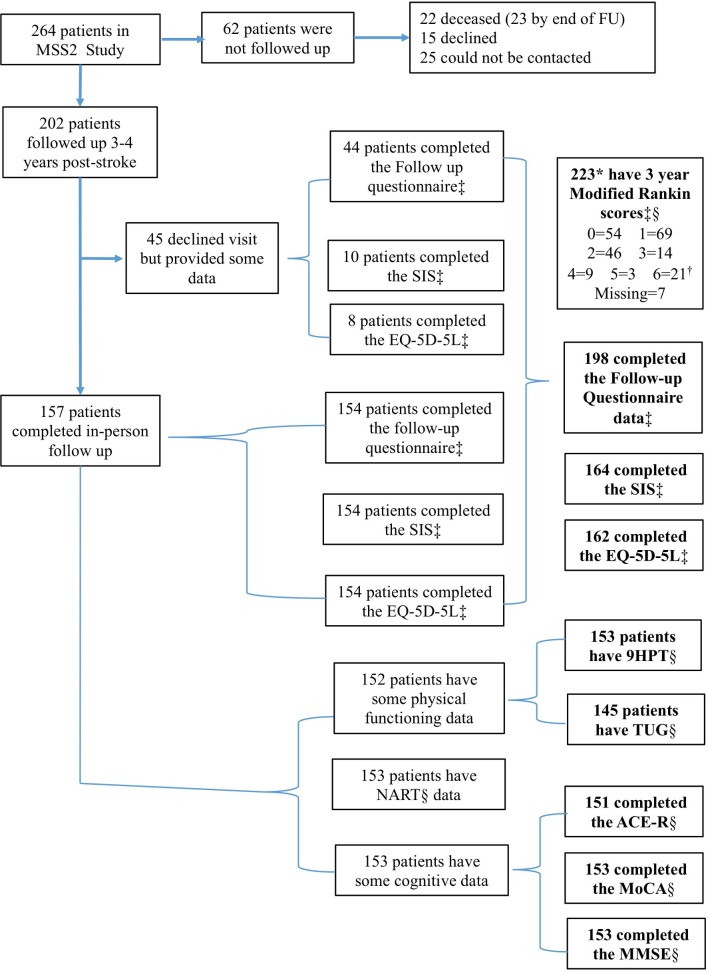
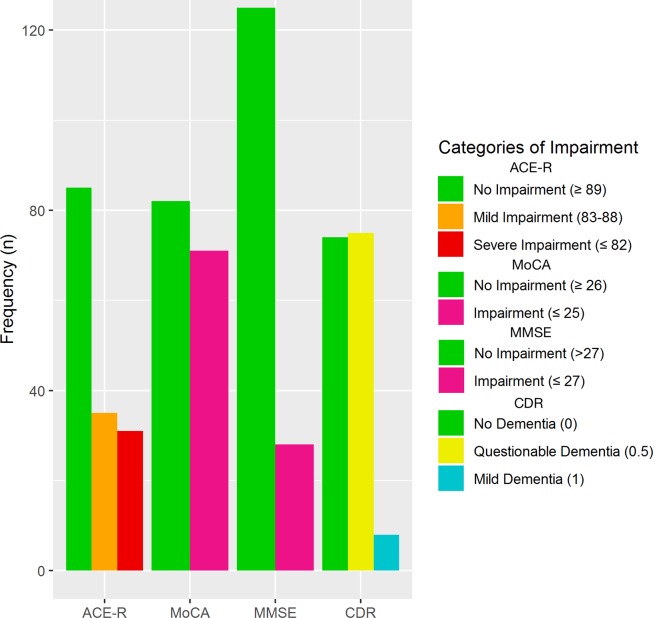
Results: We followed up 224/264 participants at 3 years (mean age at index stroke=67, 126 (56%) men, 25 non-contactable, 15 declined): 66/151 (44%) had cognitive impairment, mean ACE-R 88 (SD 9, range 54-100/100), 61/156 (39%) had depression and 26/223 (12%) were dependent (mRS=3-5). Cognitive impairment at 3 years affected all ACE-R subdomains and was associated with ACE-R 1 year (β=1.054, p<0.001) and NART (β=1.023, p<0.05). Poor physical function was associated with stroke severity (TUG, β=1.064, p<0.01) and recurrent stroke (9HPT, β=1.130, p<0.05 right, β=1.214, p<0.05 left). Higher ACE-R scores were associated with faster TUG (β=-0.279, p<0.05) and 9HPT (right β=-0.257, p<0.05; left β=-0.302, p=0.05) and inversely with dependency (mRS=3-5, OR 0.88, 95% CI 0.80 to 0.97). We adjusted analyses for demographic, stroke and known risk factors. In-person and remote assessments were highly correlated.
Conclusions: Cognitive, physical impairments and depression are common and interrelated 3 years after minor stroke. Cognitive and physical impairments require rehabilitation after minor stroke and argue for better integration of stroke and dementia services.
Keywords: activities of daily living; cognition; dependency; stroke; walking speed.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: VC reports grants from NHS Research Scotland and Chest, Heart, Stroke Scotland, which funded the study. JMW reports grants from Chest, Heart, Stroke Scotland, grants from the Sackler Foundation, European Union Horizon 2020 grant No 666881, ‘SVDs@target’, Fondation Leducq, UK Medical Research Council, Stroke Association, Alzheimer’s Society and British Heart Foundation.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous