

Effect and cost-effectiveness of pneumococcal conjugate vaccination: a global modelling analysis
- PMID: 30554762
- PMCID: PMC6293964
- DOI: 10.1016/S2214-109X(18)30422-4
Effect and cost-effectiveness of pneumococcal conjugate vaccination: a global modelling analysis
Abstract
Background: Introduction of pneumococcal conjugate vaccines (PCVs) has substantially reduced disease burden due to Streptococcus pneumoniae, a leading cause of childhood morbidity and mortality globally. However, PCVs are among the most expensive vaccines, hindering their introduction in some settings and threatening sustainability in others. We aimed to assess the effect and cost-effectiveness of introduction of 13-valent PCV (PCV13) vaccination globally.
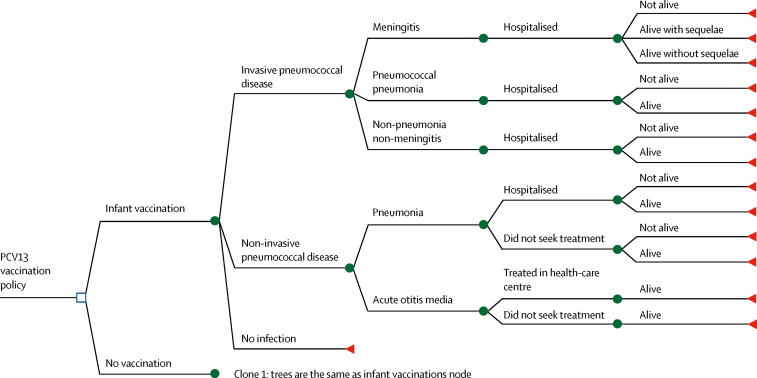
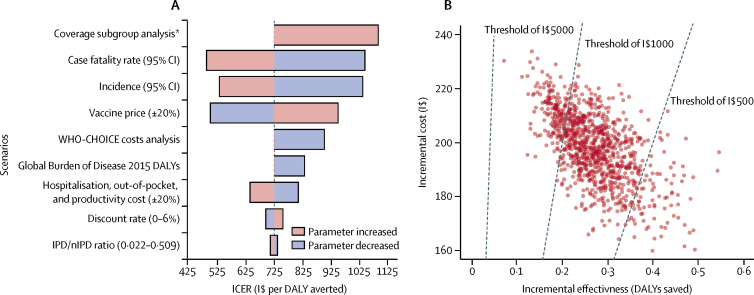
Methods: We assessed the incremental cost-effectiveness ratio of PCV13 introduction by integrating two models: an ecological model (a parsimonious, mechanistic model validated with data from post-seven-valent PCV introduction in 13 high-income settings) to predict the effect of PCV on childhood invasive pneumococcal disease, and a decision-tree model to predict a range of clinical presentations and economic outcomes under vaccination and no-vaccination strategies. The models followed 30 birth cohorts up to age 5 years in 180 countries from 2015 to 2045. One-way scenario and probabilistic sensitivity analyses were done to explore model uncertainties.
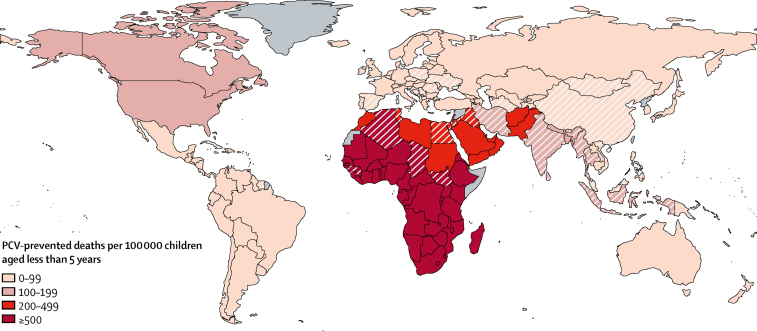
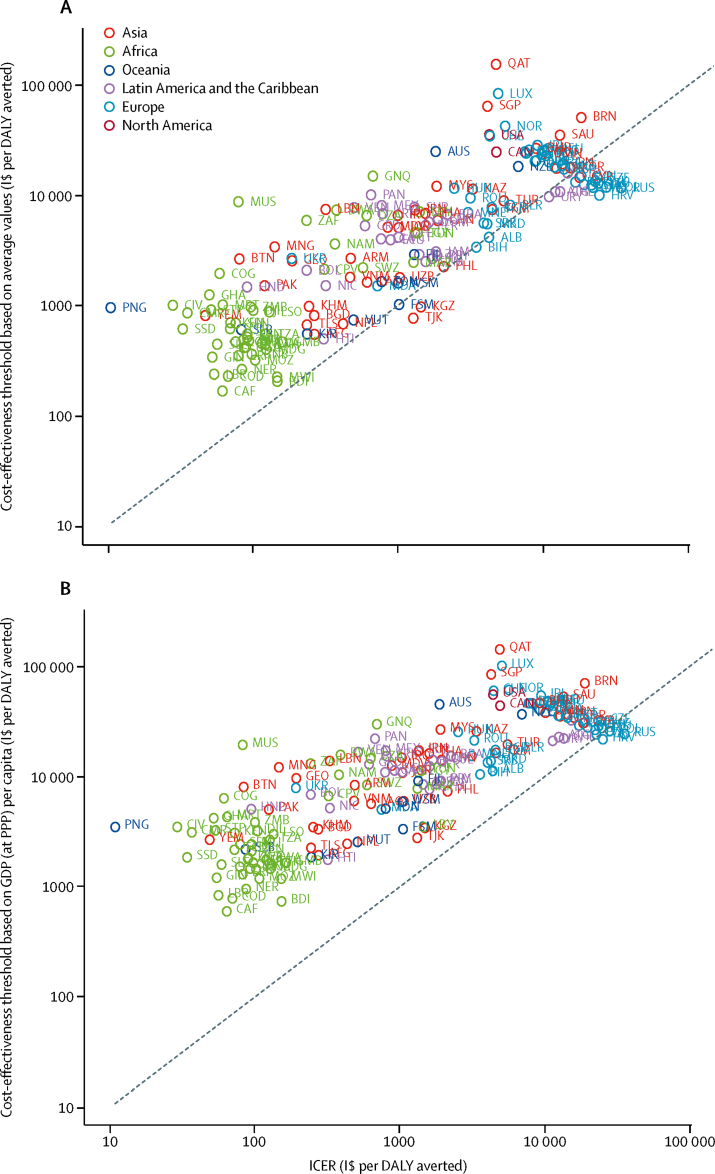
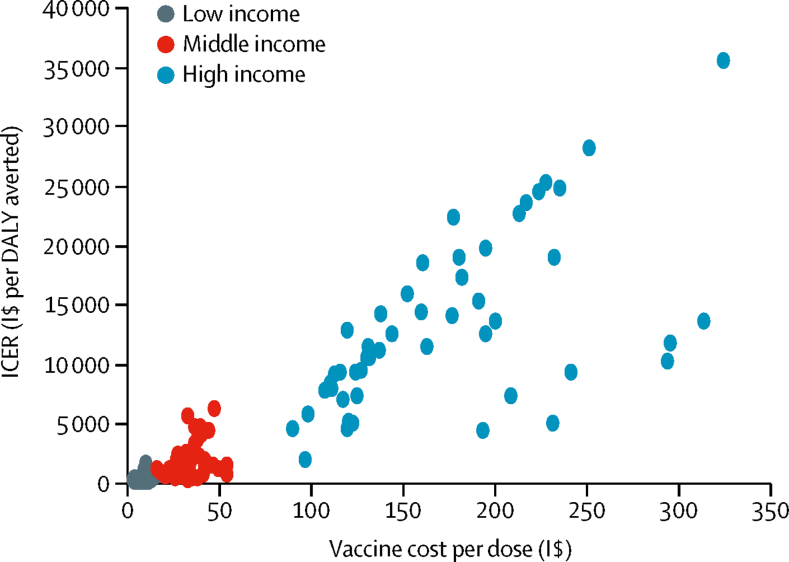
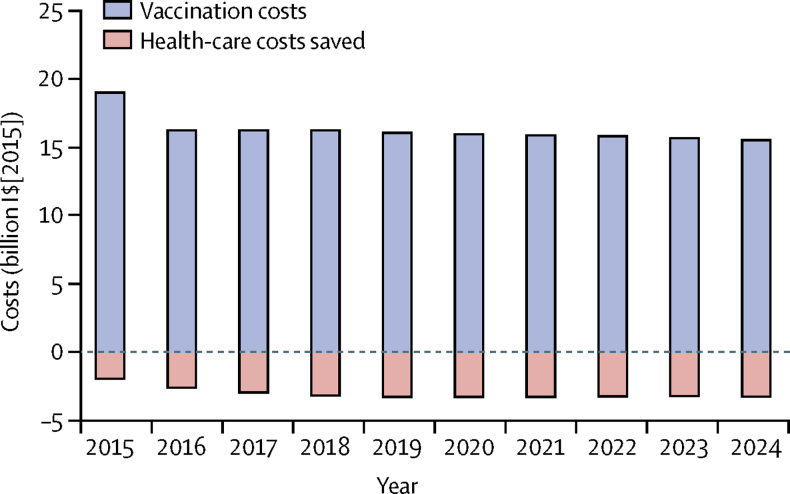
Findings: We estimate that global PCV13 use could prevent 0·399 million child deaths (95% credible interval 0·208 million to 0·711 million) and 54·6 million disease episodes (51·8 million to 58·1 million) annually. Global vaccine costs (in 2015 international dollars) of $15·5 billion could be partially offset by health-care savings of $3·19 billion (2·62 billion to 3·92 billion) and societal cost savings of $2·64 billion (2·13 billion to 3·28 billion). PCV13 use is probably cost-effective in all six UN regions. The 71 countries eligible for support from Gavi, the Vaccine Alliance, account for 83% of PCV13-preventable deaths but only 18% of global vaccination costs. The expected cost of PCV vaccination globally is around $16 billion per year.
Interpretation: Our findings highlight the value of Gavi's support for PCV introduction in low-income countries and of efforts to improve the affordability of PCVs in countries not eligible for, or transitioning from, Gavi support.
Funding: World Health Organization; Gavi, the Vaccine Alliance; and the Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- WHO Pneumococcal vaccines WHO position paper—2012. Wkly Epidemiol Rec. 2012;87:129–144. - PubMed
-
- Whitney CG. Measuring progress on preventing pneumonia deaths: are we there yet? Lancet Infect Dis. 2017;17:1100–1101. - PubMed
-
- O'Brien KL, Wolfson LJ, Watt JP. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. 2009;374:893–902. - PubMed
-
- WHO Estimated Hib and pneumococcal deaths for children under 5 years of age. 2008. http://www.who.int/immunization/monitoring_surveillance/burden/estimates...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
