

Psoriasis: Classical vs. Paradoxical. The Yin-Yang of TNF and Type I Interferon
- PMID: 30555460
- PMCID: PMC6283263
- DOI: 10.3389/fimmu.2018.02746
Psoriasis: Classical vs. Paradoxical. The Yin-Yang of TNF and Type I Interferon
Abstract
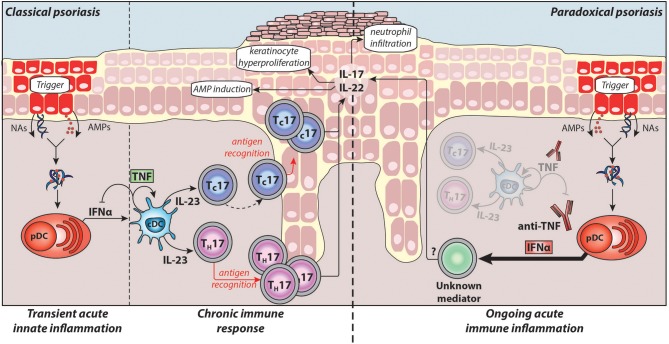
Chronic plaque psoriasis is a common debilitating skin disease. The identification of the pathogenic role of the TNF/IL-23/TH17 pathway has enabled the development of targeted therapies used in the clinic today. Particularly, TNF inhibitors have become a benchmark for the treatment of numerous chronic inflammatory diseases such as psoriasis. Although being highly effective in psoriasis treatment, anti-TNFs can themselves induce psoriasis-like skin lesions, a side effect called paradoxical psoriasis. In this review, we provide a comprehensive look at the different cellular and molecular players involved in classical plaque psoriasis and contrast its pathogenesis to paradoxical psoriasis, which is clinically similar but immunologically distinct. Classical psoriasis is a T-cell mediated autoimmune disease driven by TNF, characterised by T-cells memory, and a relapsing disease course. In contrast, paradoxical psoriasis is caused by the absence of TNF and represents an ongoing type-I interferon-driven innate inflammation that fails to elicit T-cell autoimmunity and lacks memory T cell-mediated relapses.
Keywords: IL-23; TH17; TNF; paradoxical psoriasis; plaque psoriasis; type I-interferon.
Figures
References
-
- Moreland LW, Baumgartner SW, Schiff MH, Tindall EA, Fleischmann RM, Weaver AL, et al. . Treatment of rheumatoid arthritis with a recombinant human Tumour Necrosis Factor Receptor (p75)-Fc fusion protein. N Engl J Med. (1997) 337:141–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical