

Prevalence and Incidence of Upper Respiratory Tract Infection Events Are Elevated Prior to the Development of Rheumatoid Arthritis in First-Degree Relatives
- PMID: 30555464
- PMCID: PMC6281887
- DOI: 10.3389/fimmu.2018.02771
Prevalence and Incidence of Upper Respiratory Tract Infection Events Are Elevated Prior to the Development of Rheumatoid Arthritis in First-Degree Relatives
Abstract
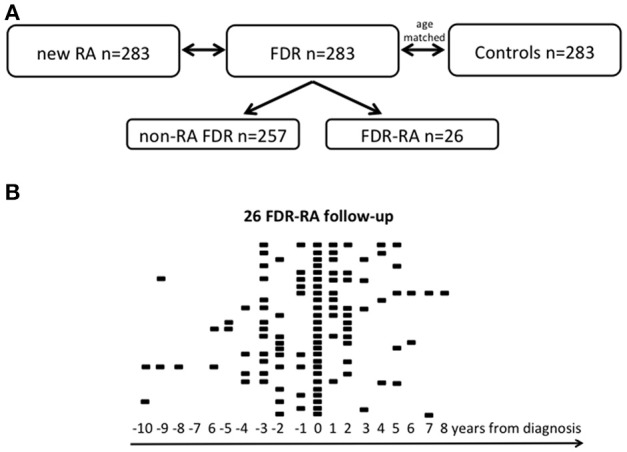
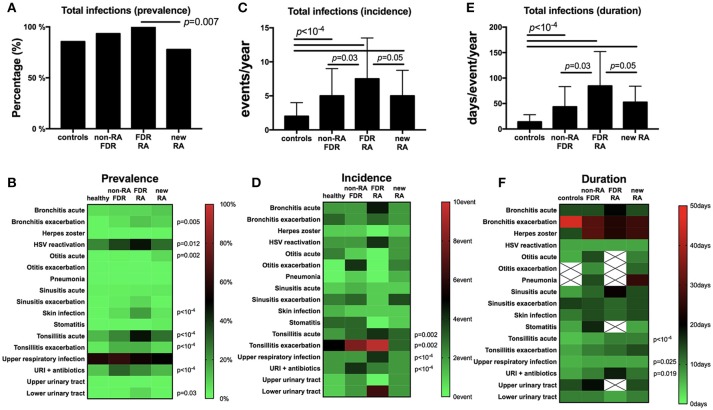
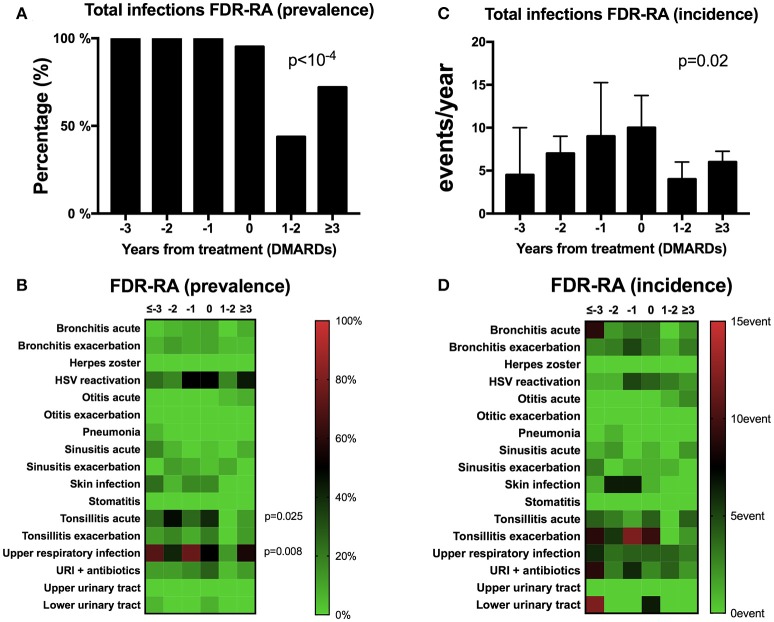
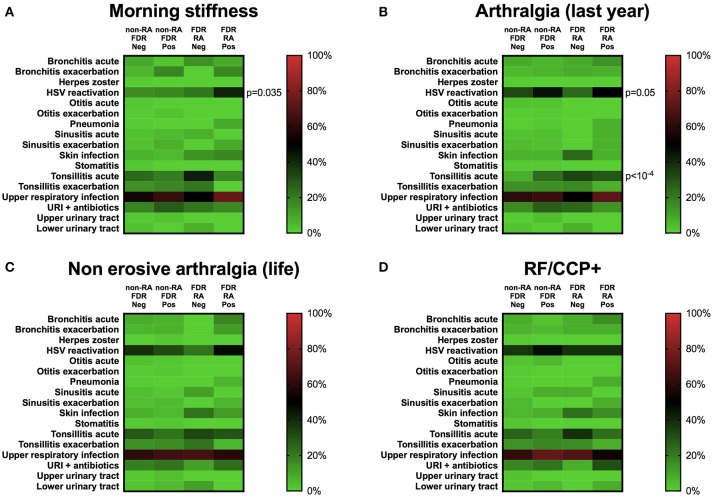
Introduction: The aim of this study was to characterize infection events in a longitudinal cohort of first-degree relatives (FDR) of probands with rheumatoid arthritis (RA) and explore their associations with RA development. To this end, newly diagnosed RA patients (n = 283), unaffected related FDR and age-matched healthy women were ascertained from the Caucasian triple women prospective Tatarstan cohort. Methods: In this cohort initiated in 1997, 26/283 (9.2%) FDR developed RA (incidence: 9.1 cases/1,000/year). At baseline and during the follow-up, information regarding infectious events (prevalence) and their incidence and duration per year were collected from all individuals. Results: Results reveal in the unaffected FDR developing RA subgroup: (i) a higher prevalence and/or incidence at baseline of upper respiratory infections (URI), otitis, tonsillitis, herpes reactivation, and skin infections; (ii) Mycoplasma sp detection was increased during pregnancy; (iii) a peak of infections started in the 3 years preceding RA onset, and thereafter decreased following RA diagnosis and treatment initiation with disease-modifying anti-rheumatic drugs (DMARDs) when considering URI, and acute tonsillitis; (iv) herpes virus reactivation, at baseline, was associated with a higher report of morning stiffness and arthralgia while independent from rheumatoid factors and anti-citrullinated peptide (CCP)2 Ab positivity; and (v) infection events represent an independent environmental factor associated with RA development. Conclusion: In conclusion, an annual increase of respiratory tract infections was found at the pre-clinical stage of RA. This could be due to alterations in the immune system that result in susceptibility to infection, controlled by DMARDs, or that the infectious events predispose to RA.
Keywords: first-degree relatives; herpes virus; infections; rheumatoid arthritis; upper respiratory tract infection symptoms.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical