

Alarming levels of antimicrobial resistance among sepsis patients admitted to ICU in a tertiary care hospital in India - a case control retrospective study
- PMID: 30555689
- PMCID: PMC6286518
- DOI: 10.1186/s13756-018-0444-8
Alarming levels of antimicrobial resistance among sepsis patients admitted to ICU in a tertiary care hospital in India - a case control retrospective study
Abstract
Background: Hospital acquired infections (HAI) are principal threats to the patients of intensive care units. An increase in the antimicrobial resistance (AMR) observed in gram negative bacteria is a great challenge to deal with. HAI and AMR lead to prolonged hospitalization and additional doses of anti-microbial treatment affecting patient's fitness and finances. Present study was undertaken to determine the pathotypes, genetic diversity and the antimicrobial resistance of E.coli in isolates from the patients admitted to intensive care unit at a tertiary care hospital in Delhi, India.
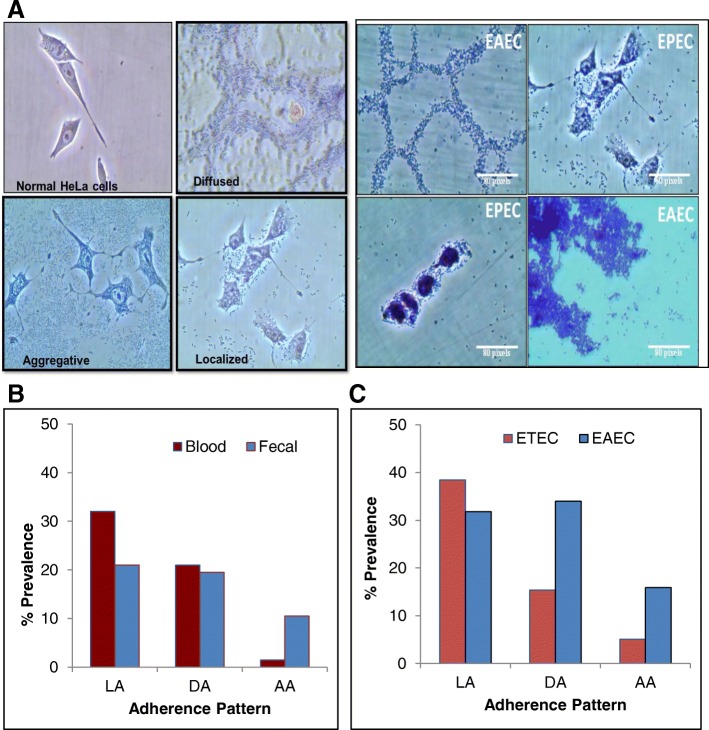
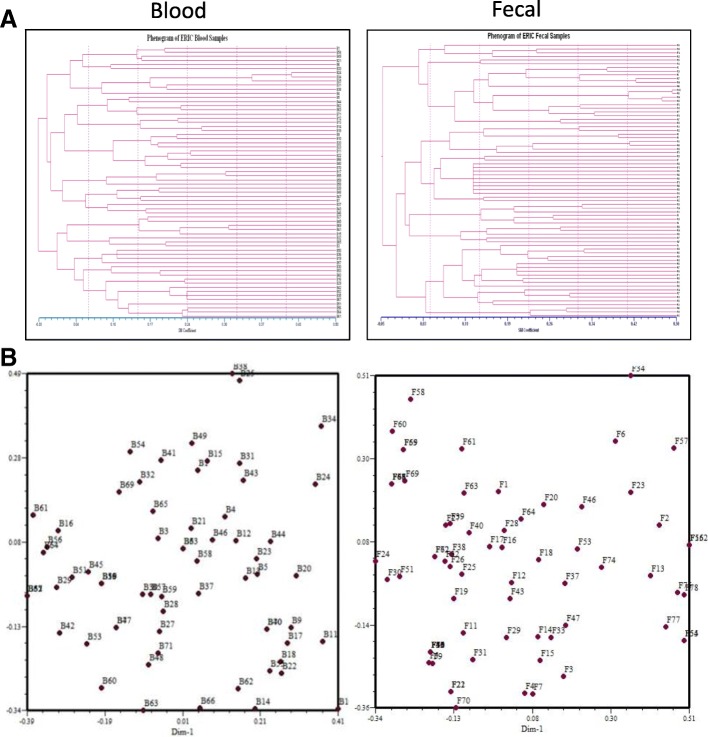
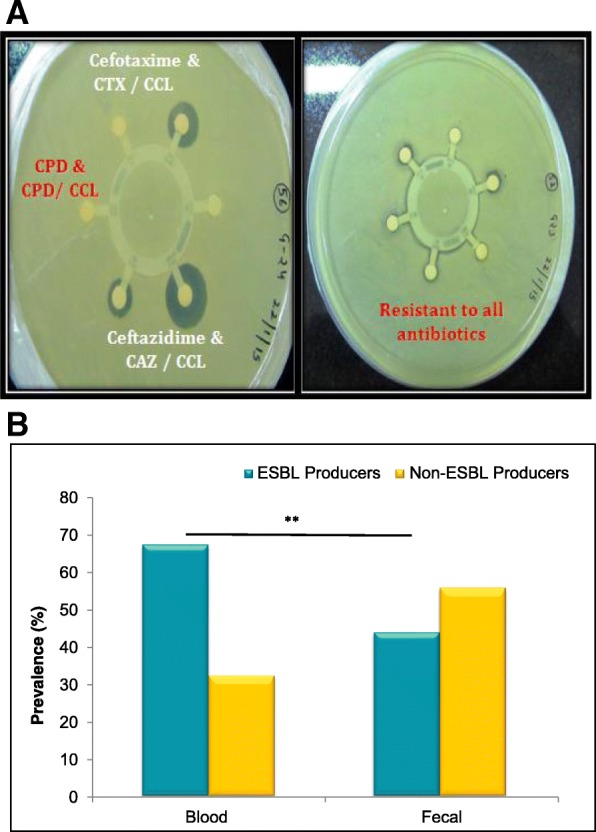
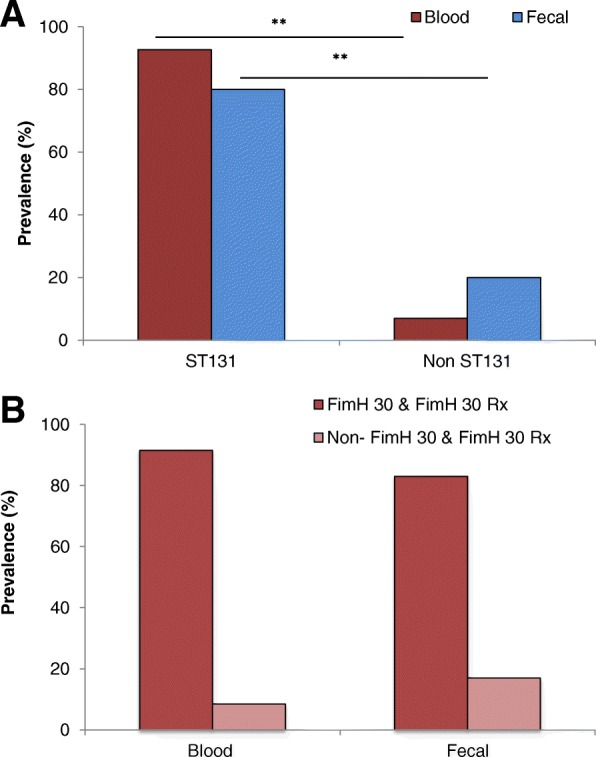
Methods: E.coli isolates (N = 77) obtained from the blood culture of patients diagnosed with sepsis and the isolates (N = 71) from the stool culture of patients admitted in intensive care unit (ICU) but not diagnosed with sepsis were investigated for their pathotypes, adherence patterns and genetic diversity by Enterobacterial Repeated Intergenic Consensus-polymerase chain reaction (ERIC-PCR). A Kirby-Bauer Disc diffusion test and antimicrobial susceptibility assays were performed according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. Extended-spectrum β-lactamase (ESBL) genes and sequence type 131 (ST131) clone were characterised genotypically by gene-specific PCRs.
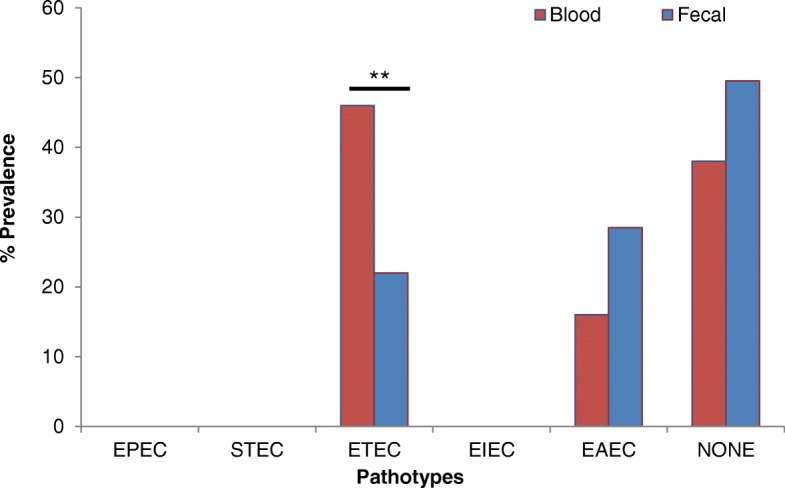
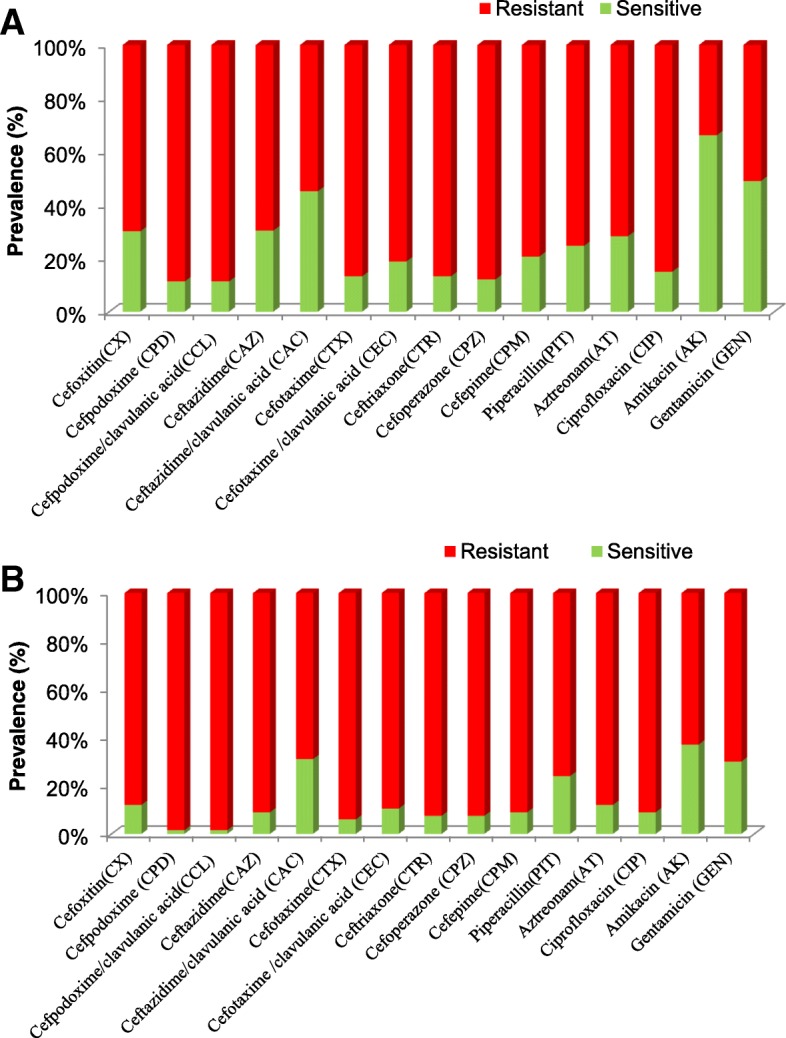
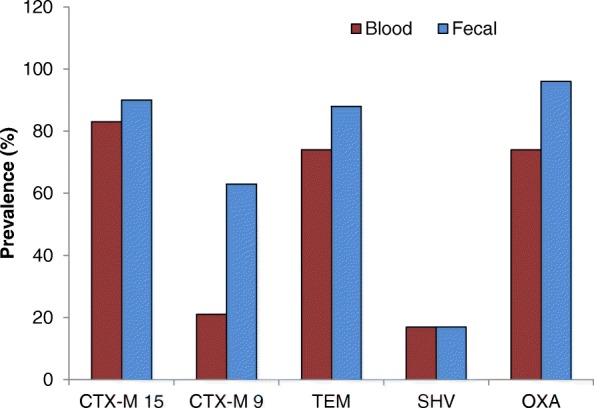
Results: Pathotypes analysis revealed 46 and 16% of the blood E.coli isolates were ETEC and EAEC respectively, in contrast to the fecal isolates wherein 22% of the isolates were ETEC and 28.5% were EAEC. EPEC, STEC and EIEC pathotypes were not detected in blood or fecal isolates. Of all the isolates studied, more than 90% of the blood and 70% of the fecal isolates were found to be resistant to cephalosporins. On the other hand, 68% of blood and 44% of the fecal isolates were found to be ESBL producers. Interestingly 83% of the blood isolates contained CTX-M15, whereas only 21% of them contained CTX-M9 genes. On the other hand CTX-M15 genes were found in 90% and CTX-M9 genes were found in 63% of the fecal isolates.
Conclusion: The antimicrobial resistant profile found in this study is alarming and poses a great threat to public health. Apparently an increased antimicrobial resistance to the extensively used cephalosporins is affecting an optimal drug therapy for patients. In addition, the presence of catheters, prolonged duration of stay in the hospital and poor hygienic conditions due to infrequent urination of the patient can lead to an additional vulnerability. Therefore continuous surveillance and rational use of antibiotics along with effective hygienic measures are urgently recommended in such settings.
Keywords: Antimicrobial resistance (AMR); Enterobacterial repeated intergenic consensus (ERIC); Escherichia coli; Intensive care unit (ICU); Pathotypes; Sepsis.
Conflict of interest statement
This project was approved by the Institutional Ethical Committee of Vardhaman Mahavir Medical College (VMCC) and Safdarjung Hospital (S.No-VMMC/SJH/Ethics/SEP-11/29) and Institute Human Ethics committee of ACBR, University of Delhi, Delhi (S.No. F50–2/Ethic.com/ACBR/2015).Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Al-Zahrani A, Alsulaimani EEA, Abbadi S. Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA. Adv Infect Dis. 2013;3(4):300–305. doi: 10.4236/aid.2013.34046. - DOI
-
- Sheng WH, et al. Impact of nosocomial infections on medical costs, hospital stay, and outcome in hospitalized patients. J Formos Med Assoc. 2005;104(5):318–326. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
