

Longitudinal exploration of in situ mock code events and the performance of cardiac arrest skills
- PMID: 30555719
- PMCID: PMC6289268
- DOI: 10.1136/bmjstel-2017-000255
Longitudinal exploration of in situ mock code events and the performance of cardiac arrest skills
Abstract
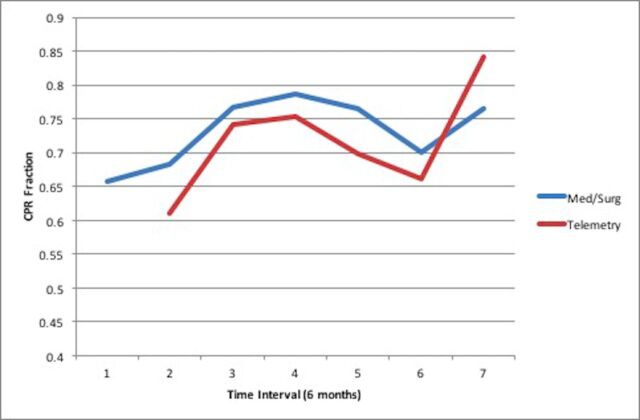
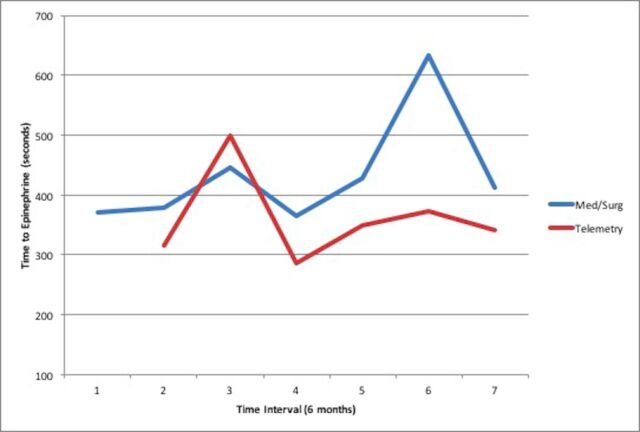
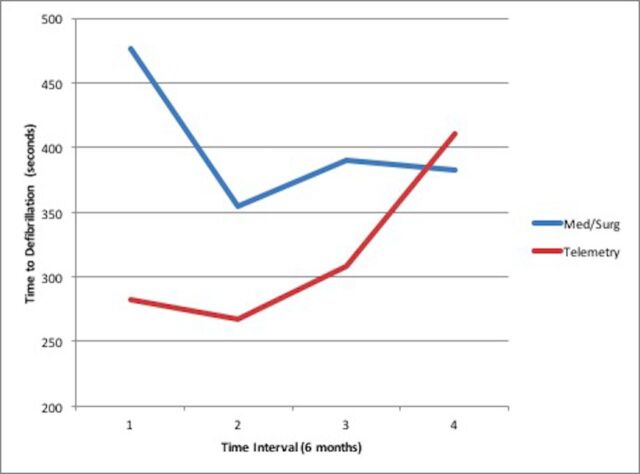
Introduction: In hospital cardiac arrest (IHCA) affects 200,000 adults in the United States each year, and resuscitative efforts are often suboptimal. The objective of this study was to determine whether a program of "mock codes" improves group-level performance of IHCA skills. Our primary outcome of interest was change in CPR fraction, and the secondary outcomes of interest were time to first dose of epinephrine and time to first defibrillation. We hypothesized that a sustained program of mock codes would translate to greater than 10% improvement in each of these core metrics over the first three years of the program.
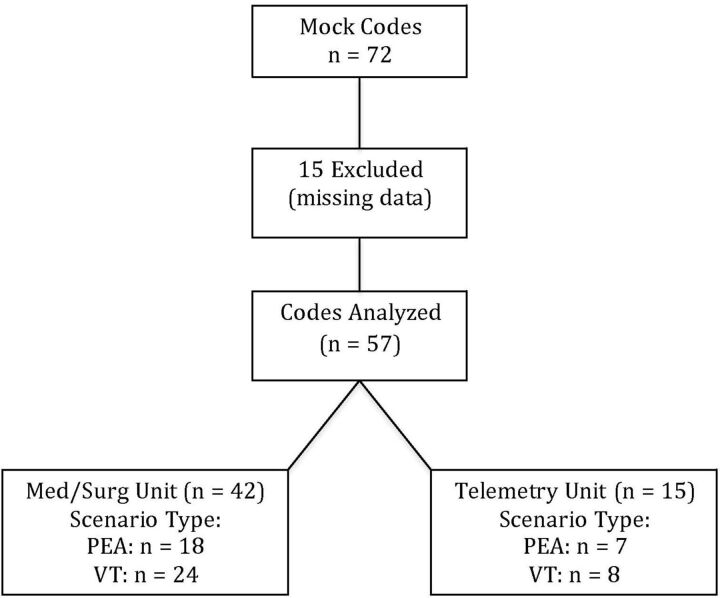
Methods: We conducted mock codes in an urban teaching hospital between August, 2012 and October, 2015. Mock codes occurred on telemetry and medical/surgical units on day and night shifts. Codes were managed by unit staff and members of the hospital's "Code Blue" team, and data were recorded by trained observers. Data were summarized using descriptive statistics, and repeated measures outcomes were calculated using a mixed effects model.
Results: Fifty-seven mock codes were included in the analysis: 42 on Medical/Surgical units and 15 on Telemetry units. CPR fraction increased by 2.9% per six-month time interval on Telemetry units, and 1.3% per time interval on Medical/Surgical units. Neither time to first epinephrine dosing nor time to defibrillation changed significantly.
Conclusions: While we observed a significant improvement in CPR fraction over the course of this program of mock codes, similar improvements were not observed for other key measures of cardiac arrest performance.
Conflict of interest statement
Competing interests statement: The authors of this manuscript have no competing interests.
Figures
Similar articles
-
Use of automated external defibrillators in cardiac arrest: an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(19):1-29. Epub 2005 Dec 1. Ont Health Technol Assess Ser. 2005. PMID: 23074470 Free PMC article.
-
Impact of a pediatric primary care office-based mock code program on physician and staff confidence to perform life-saving skills.Pediatr Emerg Care. 2006 Jun;22(6):415-22. doi: 10.1097/01.pec.0000221342.11626.12. Pediatr Emerg Care. 2006. PMID: 16801842 Clinical Trial.
-
The Impact of Mock Code Simulation on the Resuscitation Practice and Patient Outcome for Children With Cardiopulmonary Arrest.Cureus. 2020 Jul 15;12(7):e9197. doi: 10.7759/cureus.9197. Cureus. 2020. PMID: 32789097 Free PMC article.
-
A cumulative meta-analysis of the effectiveness of defibrillator-capable emergency medical services for victims of out-of-hospital cardiac arrest.Ann Emerg Med. 1999 Oct;34(4 Pt 1):517-25. Ann Emerg Med. 1999. PMID: 10499952
-
Pediatric In-Hospital Cardiac Arrest and Cardiopulmonary Resuscitation in the United States: A Review.JAMA Pediatr. 2021 Mar 1;175(3):293-302. doi: 10.1001/jamapediatrics.2020.5039. JAMA Pediatr. 2021. PMID: 33226408 Free PMC article. Review.
Cited by
-
Use of In Situ Simulation to Improve Emergency Department Readiness for the COVID-19 Pandemic.Prehosp Disaster Med. 2021 Feb;36(1):6-13. doi: 10.1017/S1049023X2000134X. Epub 2020 Oct 21. Prehosp Disaster Med. 2021. PMID: 33081859 Free PMC article.
-
In situ simulation for cardiopulmonary resuscitation training: A systematic review.Resusc Plus. 2025 Jan 3;21:100863. doi: 10.1016/j.resplu.2024.100863. eCollection 2025 Jan. Resusc Plus. 2025. PMID: 39897060 Free PMC article. Review.