

Reducing acute kidney injury incidence and progression in a large teaching hospital
- PMID: 30555931
- PMCID: PMC6267307
- DOI: 10.1136/bmjoq-2017-000308
Reducing acute kidney injury incidence and progression in a large teaching hospital
Abstract
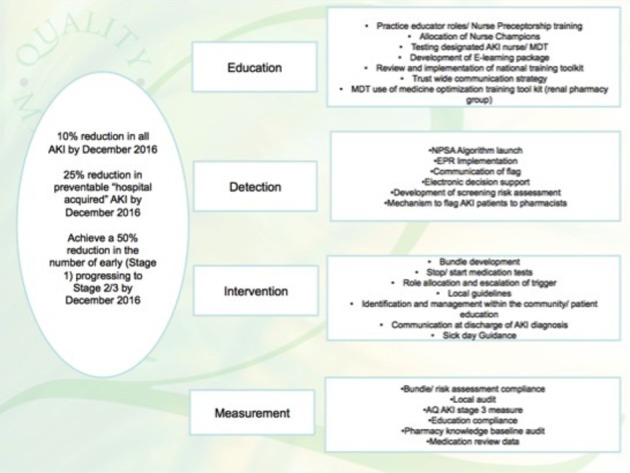
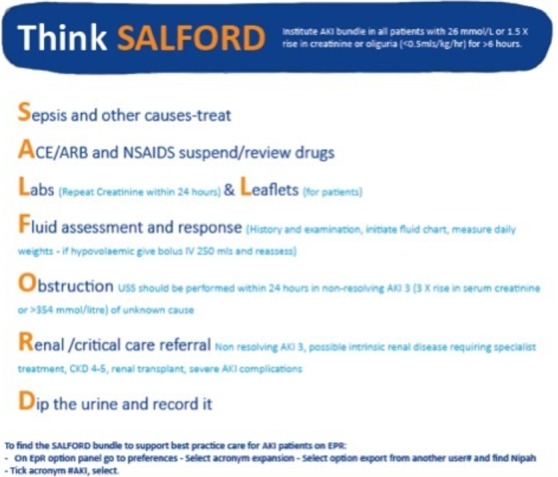
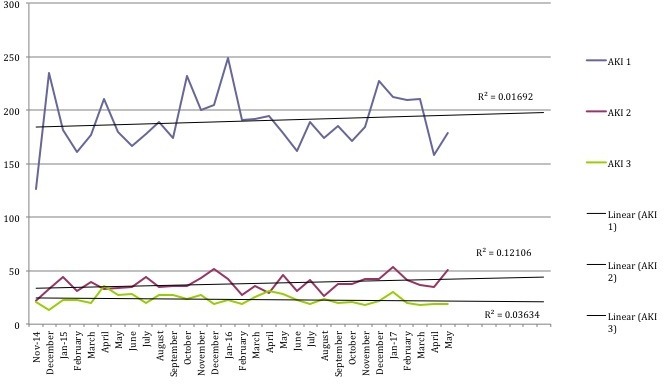
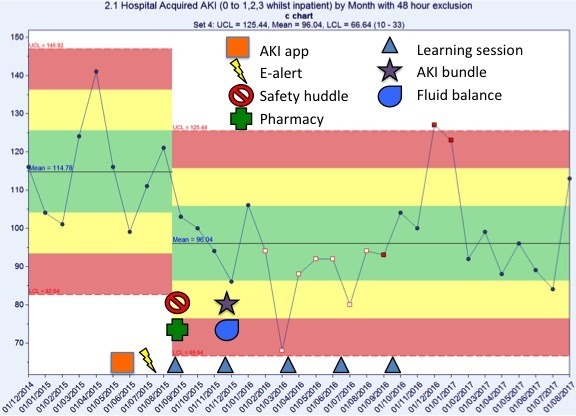
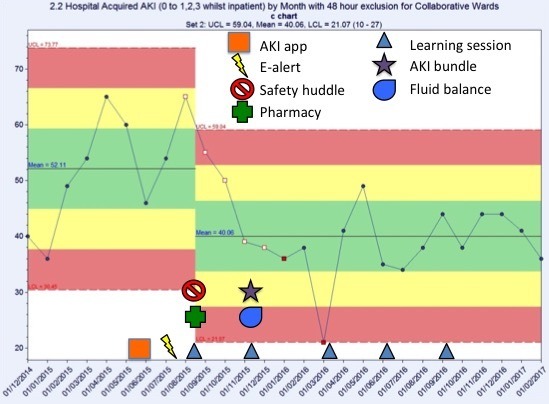
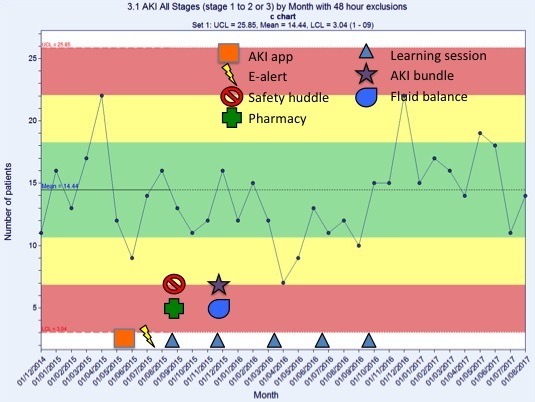
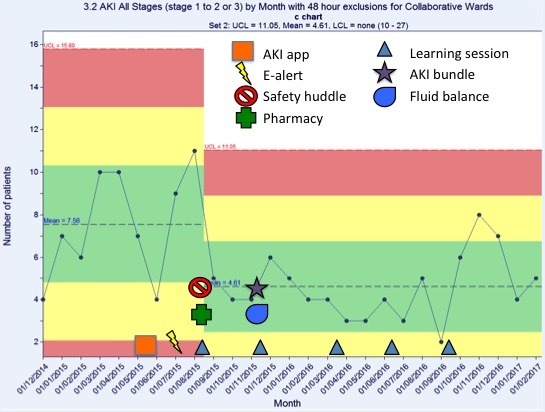
Acute kidney injury (AKI) is a common syndrome that is associated with significant mortality and cost. The Quality Improvement AKI Collaborative at Salford Royal Foundation Trust was established to review and improve both the recognition and management of AKI. This was a whole-system intervention to tackle AKI implemented as an alternative to employing separate AKI nurses. Our aims were to reduce the overall incidence of AKI by 10%, to reduce hospital-acquired AKI by 25% and to reduce the progression of AKI from stage 1 to stage 2 or 3 by 50%. From 2014 to 2016, several multifaceted changes were introduced. These included system changes, such as inserting an e-alert for AKI into the electronic patient record, an online educational package and face-to-face teaching for AKI, and AKI addition to daily safety huddles. On 10 Collaborative wards, development of an AKI care bundle via multidisciplinary team (MDT) plan, do, study, act testing occurred. Results showed a 15.6% reduction in hospital-wide-acquired AKI, with a 22.3% reduction on the collaborative wards. Trust-wide rates of progression of AKI 1 to AKI 2 or 3 showed normal variation, whereas there was a 48.5% reduction in AKI progression on the Collaborative wards. This implies that e-alerts were ineffective in isolation. The Collaborative wards' results were a product of the educational support, bundle and heightened awareness of AKI. A number of acute hospitals have demonstrated impactful successes in AKI reduction centred on a dedicated AKI nurse model plus e-alerting with supporting changes. This project adds value by highlighting another approach that does not require a new post with attendant rolling costs and risks. We believe that our approach increased our efficacy in acute care in our front-line teams by concentrating on embedding improved recognition and actions across the MDT.
Keywords: collaborative, breakthrough groups; continuous quality improvement; control charts/run charts; healthcare quality improvement; quality improvement.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Sterwart J, Findlay G, Smith N, et al. . Acute kidney injury: adding insult to injury. Natl Confid Enq into Patient Outcomes Death 2009:1–22.
-
- Institute for Healthcare Improvement. The breakthrough series. Innovation 2003. –1.
-
- Public Health England. Salford health profile 2015. 2015. https://www.salford.gov.uk/media/387768/healthprofile_2015_salford.pdf.
LinkOut - more resources
Full Text Sources