

Deep anterior lamellar keratoplasty: A surgeon's guide
- PMID: 30555961
- PMCID: PMC6276733
- DOI: 10.1016/j.joco.2018.06.004
Deep anterior lamellar keratoplasty: A surgeon's guide
Abstract
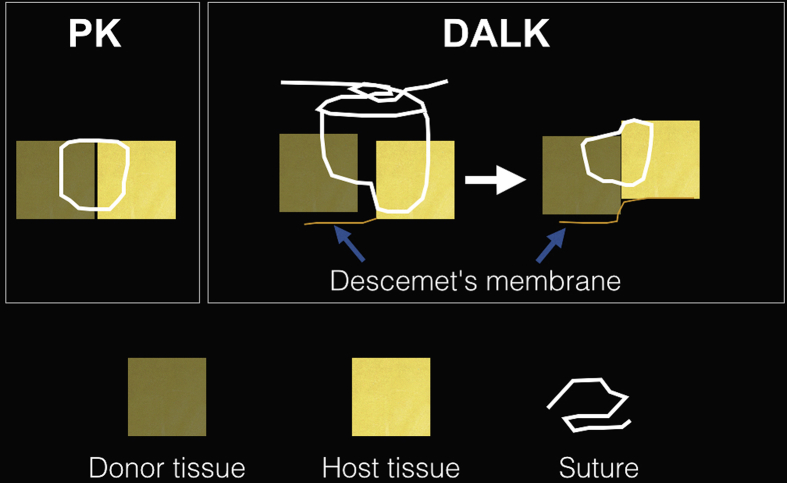
Purpose: To review and highlight important practical aspects of deep anterior lamellar keratoplasty (DALK) surgery and provide some useful tips for surgeons wishing to convert to this procedure from the conventional penetrating keratoplasty (PK) technique.
Methods: In this narrative review, the procedure of DALK is described in detail. Important pre, intra, and postoperative considerations are discussed with illustrative examples for better understanding. A comprehensive literature review was conducted in PubMed/Medline from January 1995 to July 2017 to identify original studies in English language regarding DALK. The primary endpoint of this review was the narrative description of surgical steps for DALK, its pitfalls, and management of common intraoperative complications.
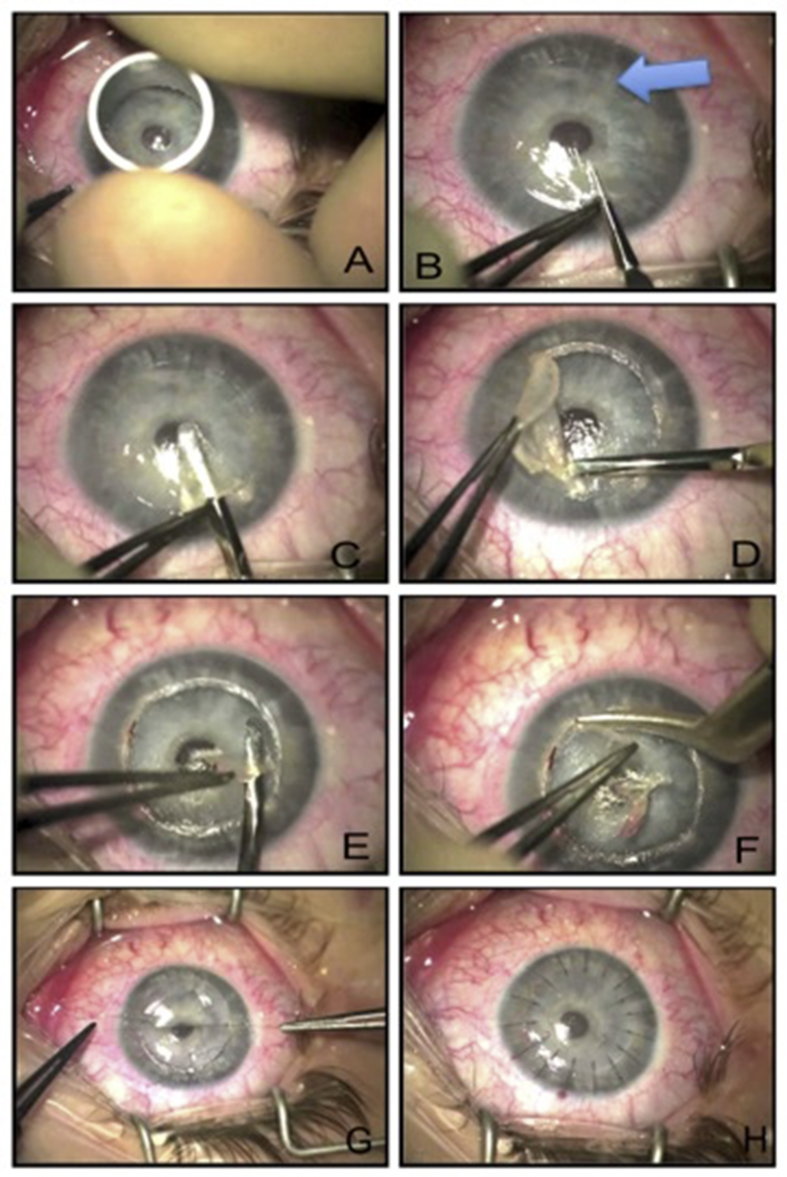
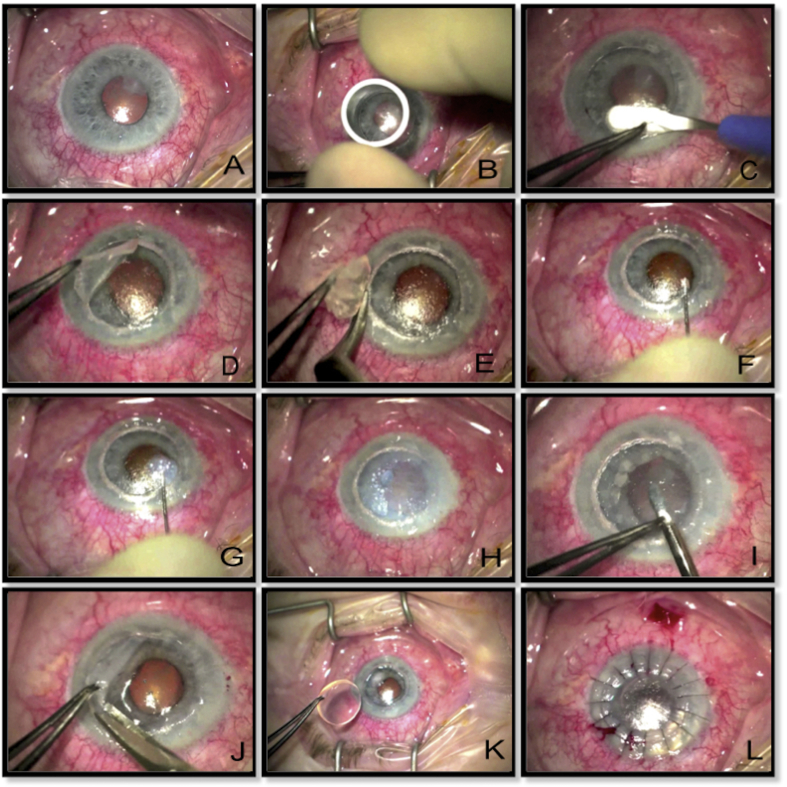
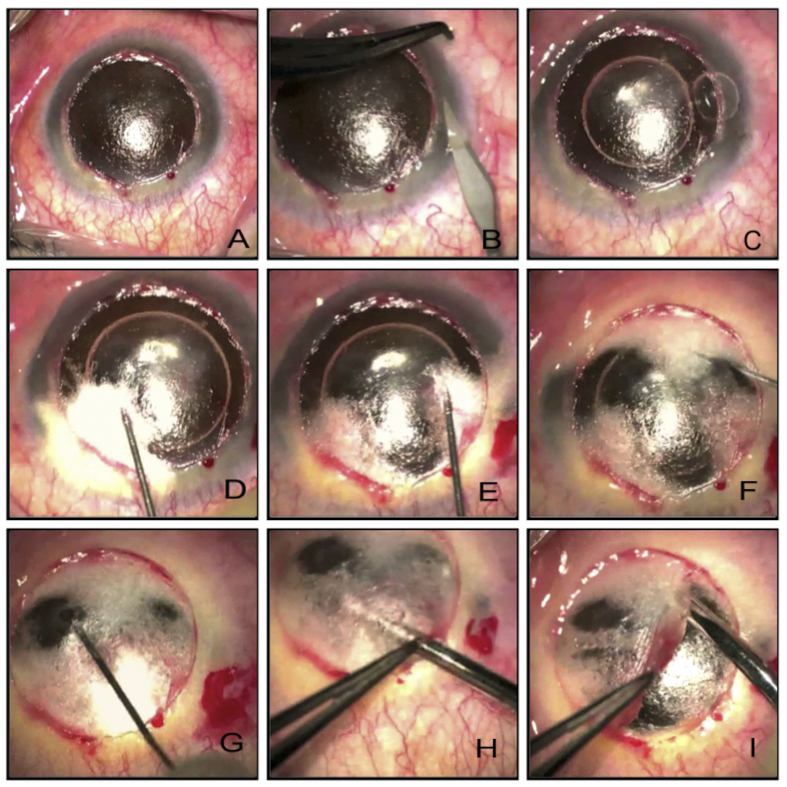
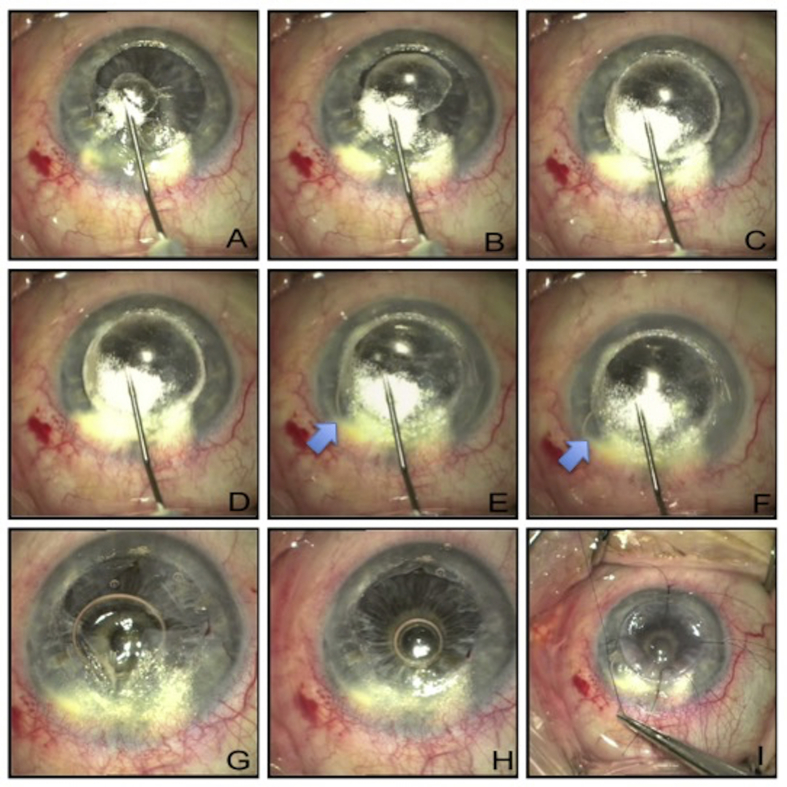
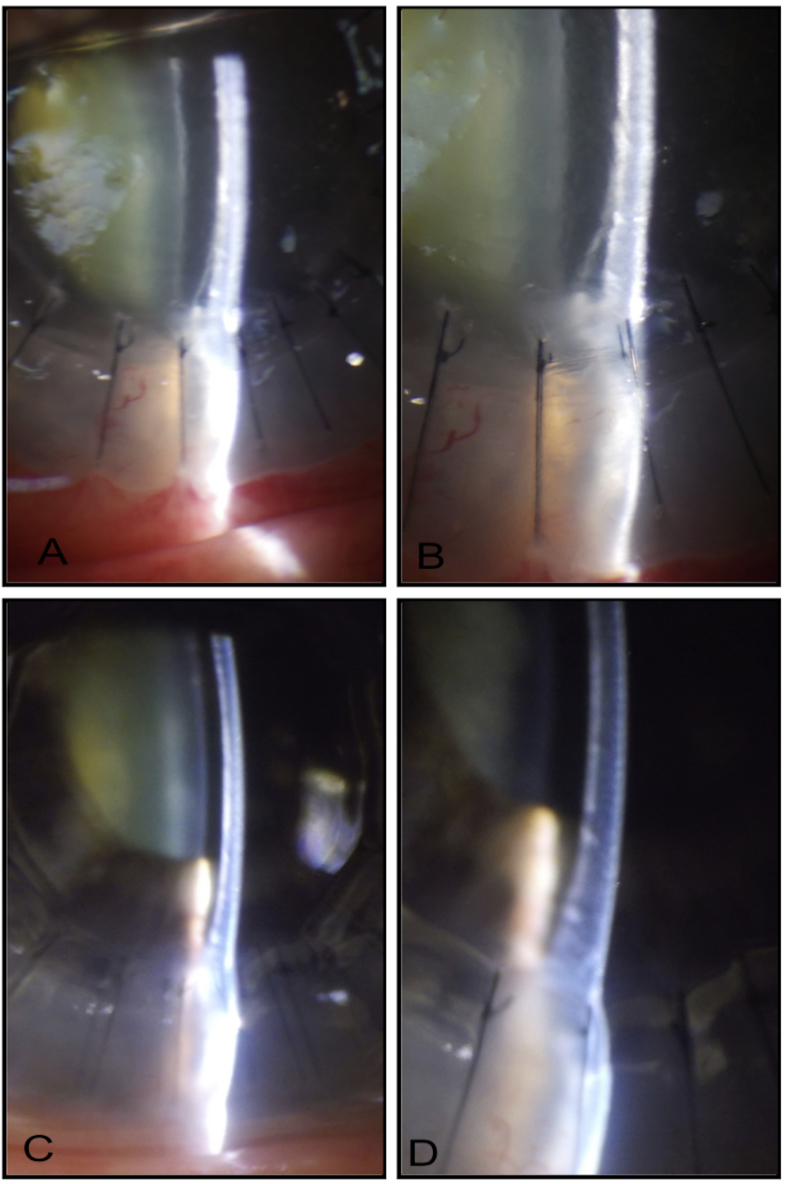
Results: A standard DALK procedure can be successfully performed taking into consideration factors such as age, ophthalmic co-morbidities, status of the crystalline lens, retina, and intraocular pressure. Careful trephination and dissection of the host cornea employing appropriate technique (such as big bubble technique, manual dissection, visco-dissection, etc.) suitable for the specific case is important to achieve good postoperative outcomes. Prompt identification of intraoperative complications such as double bubble, micro and macroperforations, etc. are vital to change the management strategies.
Conclusion: Although there is a steep learning curve for DALK procedure, considering details and having insight into the management of intraoperative issues facilitates learning and reduces complication rates.
Keywords: DALK; Keratoplasty; Lamellar corneal transplant.
Figures

References
-
- Castroviejo R. Keratoplasty in treatment of keratoconus. Arch Ophthalmol. 1949;42(6):776–800. - PubMed
-
- Coster D.J., Lowe M.T., Keane M.C. A comparison of lamellar and penetrating keratoplasty outcomes: a registry study. Ophthalmology. 2014;121(5):979–987. - PubMed
-
- Jaycock P.D., Jones M.N., Males J. Outcomes of same-sizing versus oversizing donor trephines in keratoconic patients undergoing first penetrating keratoplasty. Ophthalmology. 2008;115(2):268–275. - PubMed
-
- Watson S.L., Tuft S.J., Dart J.K. Patterns of rejection after deep lamellar keratoplasty. Ophthalmology. 2006;113(4):556–560. - PubMed
-
- Thompson R.W., Jr., Price M.O., Bowers P.J., Price F.W., Jr. Long-term graft survival after penetrating keratoplasty. Ophthalmology. 2003;110(7):1396–1402. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
