

Home-based Cognitive Prehabilitation in Older Surgical Patients: A Feasibility Study
- PMID: 30557230
- PMCID: PMC6652226
- DOI: 10.1097/ANA.0000000000000569
Home-based Cognitive Prehabilitation in Older Surgical Patients: A Feasibility Study
Abstract
Background: Cognitive training is beneficial in various clinical settings, although its perioperative feasibility and impact remain unknown. The objective of this pilot study was to determine the feasibility of home-based cognitive prehabilitation before major surgery in older adults.
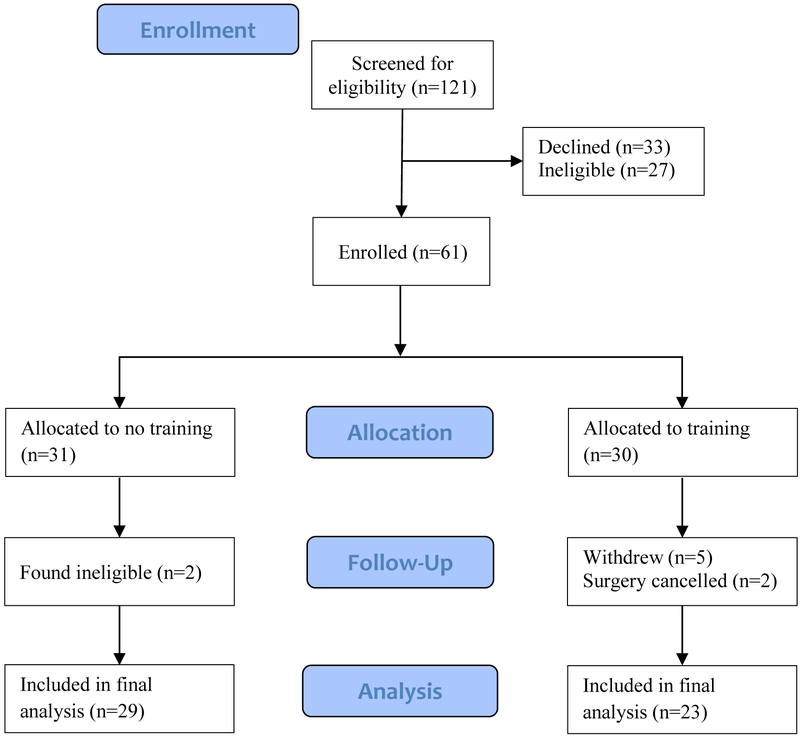
Materials and methods: Sixty-one patients were enrolled, randomized, and allocated to either a home-based preoperative cognitive training regimen or no training before surgery. Outcomes included postoperative delirium incidence (primary outcome; assessed with the 3D-Confusion Assessment Method), perioperative cognitive function based on NIH Toolbox measures, hospital length of stay, and physical therapy session participation. Reasons for declining enrollment were reported, as were reasons for opting out of the training program.
Results: Postoperative delirium incidence was 6 of 23 (26%) in the prehabilitation group compared with 5 of 29 (17%) in the control group (P=0.507). There were no significant differences between groups in NIH Toolbox cognitive function scoring, hospital length of stay, or physical therapy participation rates. Study feasibility data were also collected and reported. The most common reasons for declining enrollment were lack of computer access (n=19), time commitment (n=9), and feeling overwhelmed (n=9). In the training group, only 5 of 29 (17%) included patients were able to complete the prescribed 7 days of training, and 14 of 29 (48%) opted out of training once home. Most common reasons were feeling overwhelmed (n=4) and computer difficulties (n=3).
Conclusions: Short-term, home-based cognitive training before surgery is unlikely to be feasible for many older patients. Barriers to training include feeling overwhelmed, technical issues with training, and preoperative time commitment.
Conflict of interest statement
Comment in
-
Cognitive Prehabilitation: Supercharged Mind or Wishful Thinking?J Neurosurg Anesthesiol. 2019 Apr;31(2):174-176. doi: 10.1097/ANA.0000000000000579. J Neurosurg Anesthesiol. 2019. PMID: 30664040 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
