

Surgery and protontherapy in Grade I and II skull base chondrosarcoma: A comparative retrospective study
- PMID: 30557382
- PMCID: PMC6296545
- DOI: 10.1371/journal.pone.0208786
Surgery and protontherapy in Grade I and II skull base chondrosarcoma: A comparative retrospective study
Abstract
Objective: Skull base chondrosarcoma is a rare tumour usually treated by surgery and proton therapy. However, as mortality rate is very low and treatment complications are frequent, a less aggressive therapeutic strategy could be considered. The objective of this study was to compare the results of surgery only vs surgery and adjuvant proton therapy, in terms of survival and treatment adverse effects, based on a retrospective series.
Methods: Monocentric retrospective study at a tertiary care centre. All patients treated for a skull base grade I and II chondrosarcoma were included. We collected data concerning surgical and proton therapy treatment and up-to-date follow-up, including Common Terminology Criteria for Adverse Events (CTCAE) scores.
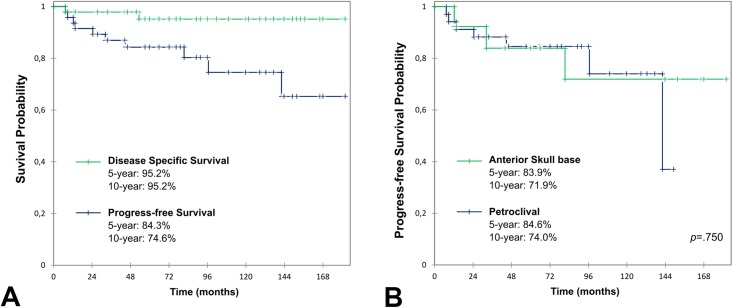
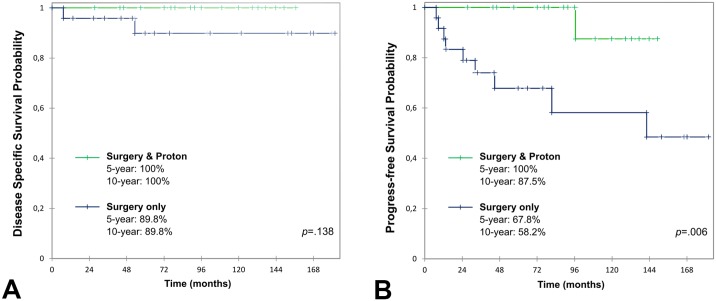
Results: 47 patients (23M/24F) were operated on between 2002 and 2015; mean age at diagnosis was 47 years-old (10-85). Petroclival and anterior skull base locations were found in 34 and 13 patients, respectively. Gross total resection was achieved in 17 cases (36%) and partial in 30 (64%). Adjuvant proton therapy (mean total dose 70 GyRBE,1.8 GyRBE/day) was administered in 23 cases. Overall mean follow-up was 91 months (7-182). Of the patients treated by surgery only, 8 (34%) experienced residual tumour progression (mean delay 51 months) and 5 received second-line proton therapy. Adjuvant proton therapy was associated with a significantly lower rate of relapse (11%; p = 0.01). There was no significant difference in 10-year disease specific survival between patients initially treated with or without adjuvant proton therapy (100% vs 89.8%, p = 0.14). Difference in high-grade toxicity was not statistically significant between patients in both groups (25% (7) vs 11% (5), p = 0.10). The most frequent adverse effect of proton therapy was sensorineural hearing loss (39%).
Conclusion: Long-term disease specific survival was not significantly lower in patients without adjuvant proton therapy, but they experienced less adverse effects. We believe a surgery only strategy could be discussed, delaying as much as possible proton therapy in cases of relapse. Further prospective studies are needed to validate this more conservative strategy in skull base chondrosarcoma.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Barnes L. Pathology and genetics of head and neck tumours: IARC; 2005.
-
- Berkmen YM, Blatt ES. Cranial and intracranial cartilaginous tumours. Clin Radiol. 1968;19(3):327–33. - PubMed
-
- Coca-Pelaz A, Rodrigo JP, Triantafyllou A, Hunt JL, Fernandez-Miranda JC, Strojan P, et al. Chondrosarcomas of the head and neck. Eur Arch Otorhinolaryngol. 2014;271(10):2601–9. 10.1007/s00405-013-2807-3 - DOI - PubMed
-
- Koch BB, Karnell LH, Hoffman HT, Apostolakis LW, Robinson RA, Zhen W, et al. National cancer database report on chondrosarcoma of the head and neck. Head Neck. 2000;22(4):408–25. - PubMed
-
- Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer. 1977;40(2):818–31. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
