

Cost-Effectiveness of Buprenorphine-Naloxone Versus Extended-Release Naltrexone to Prevent Opioid Relapse
- PMID: 30557443
- PMCID: PMC6581635
- DOI: 10.7326/M18-0227
Cost-Effectiveness of Buprenorphine-Naloxone Versus Extended-Release Naltrexone to Prevent Opioid Relapse
Abstract
Background: Not enough evidence exists to compare buprenorphine-naloxone with extended-release naltrexone for treating opioid use disorder.
Objective: To evaluate the cost-effectiveness of buprenorphine-naloxone versus extended-release naltrexone.
Design: Cost-effectiveness analysis alongside a previously reported randomized clinical trial of 570 adults in 8 U.S. inpatient or residential treatment programs.
Data sources: Study instruments.
Target population: Adults with opioid use disorder.
Time horizon: 24-week intervention with an additional 12 weeks of observation.
Perspective: Health care sector and societal.
Interventions: Buprenorphine-naloxone and extended-release naltrexone.
Outcome measures: Incremental costs combined with incremental quality-adjusted life-years (QALYs) and incremental time abstinent from opioids.
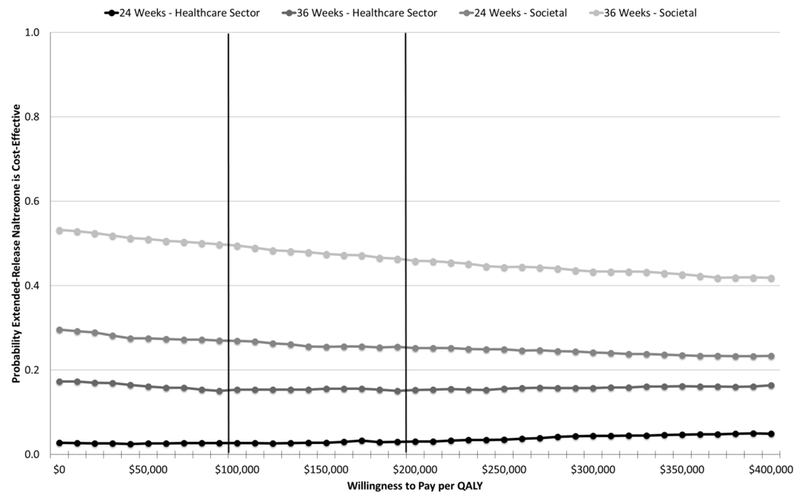
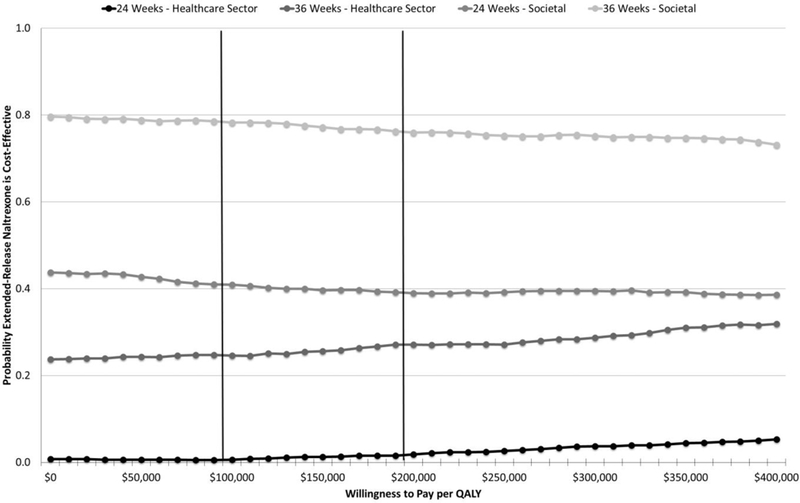
Results of base-case analysis: Use of the health care sector perspective and a willingness-to-pay threshold of $100 000 per QALY showed buprenorphine-naloxone to be preferable to extended-release naltrexone in 97% of bootstrap replications at 24 weeks and in 85% at 36 weeks. Similar results were obtained with incremental time abstinent from opioids as an outcome and with use of the societal perspective.
Results of sensitivity analysis: The base-case results were sensitive to the cost of the 2 treatments and the success of randomized treatment initiation.
Limitation: Relatively short follow-up for a chronic condition, substantial missing data, no information on patient out-of-pocket and social service costs.
Conclusion: Buprenorphine-naloxone is preferred to extended-release naltrexone as first-line treatment when both options are clinically appropriate and patients require detoxification before initiating extended-release naltrexone.
Primary funding source: National Institute on Drug Abuse, National Institutes of Health.
Figures
Comment in
-
Being Explicit About Decisions: Prescribe Medications for Opioid Use Disorder on the Basis of Proven Effectiveness, Not Beliefs.Ann Intern Med. 2019 Jan 15;170(2):127-128. doi: 10.7326/M18-3293. Epub 2018 Dec 18. Ann Intern Med. 2019. PMID: 30557444 No abstract available.
Similar articles
-
Cost-effectiveness of long-term outpatient buprenorphine-naloxone treatment for opioid dependence in primary care.J Gen Intern Med. 2012 Jun;27(6):669-76. doi: 10.1007/s11606-011-1962-8. Epub 2012 Jan 4. J Gen Intern Med. 2012. PMID: 22215271 Free PMC article.
-
Cost-effectiveness of Treatments for Opioid Use Disorder.JAMA Psychiatry. 2021 Jul 1;78(7):767-777. doi: 10.1001/jamapsychiatry.2021.0247. JAMA Psychiatry. 2021. PMID: 33787832 Free PMC article.
-
Effectiveness of Injectable Extended-Release Naltrexone vs Daily Buprenorphine-Naloxone for Opioid Dependence: A Randomized Clinical Noninferiority Trial.JAMA Psychiatry. 2017 Dec 1;74(12):1197-1205. doi: 10.1001/jamapsychiatry.2017.3206. JAMA Psychiatry. 2017. PMID: 29049469 Free PMC article. Clinical Trial.
-
Prior National Drug Abuse Treatment Clinical Trials Network (CTN) opioid use disorder trials as background and rationale for NIDA CTN-0100 "optimizing retention, duration and discontinuation strategies for opioid use disorder pharmacotherapy (RDD)".Addict Sci Clin Pract. 2021 Mar 6;16(1):15. doi: 10.1186/s13722-021-00223-z. Addict Sci Clin Pract. 2021. PMID: 33676577 Free PMC article. Review.
-
A pharmaceutical industry perspective on the economics of treatments for alcohol and opioid use disorders.Ann N Y Acad Sci. 2014 Oct;1327(1):112-30. doi: 10.1111/nyas.12538. Epub 2014 Sep 18. Ann N Y Acad Sci. 2014. PMID: 25236185 Free PMC article. Review.
Cited by
-
Econometric Issues in Prospective Economic Evaluations Alongside Clinical Trials: Combining the Nonparametric Bootstrap With Methods That Address Missing Data.Epidemiol Rev. 2022 Dec 21;44(1):67-77. doi: 10.1093/epirev/mxac006. Epidemiol Rev. 2022. PMID: 36104860 Free PMC article. Review.
-
Modeling the cost-effectiveness and impact on fatal overdose and initiation of buprenorphine-naloxone treatment at syringe service programs.Addiction. 2022 Oct;117(10):2635-2648. doi: 10.1111/add.15883. Epub 2022 Apr 3. Addiction. 2022. PMID: 35315148 Free PMC article.
-
Oleanolic Acid Attenuates Morphine Withdrawal Symptoms in Rodents: Association with Regulation of Dopamine Function.Drug Des Devel Ther. 2021 Aug 24;15:3685-3696. doi: 10.2147/DDDT.S326583. eCollection 2021. Drug Des Devel Ther. 2021. PMID: 34465980 Free PMC article.
-
Estimated Clinical Outcomes and Cost-effectiveness Associated With Provision of Addiction Treatment in US Primary Care Clinics.JAMA Netw Open. 2023 Apr 3;6(4):e237888. doi: 10.1001/jamanetworkopen.2023.7888. JAMA Netw Open. 2023. PMID: 37043198 Free PMC article.
-
Cost-Effectiveness of Implementation Facilitation to Promote Emergency Department-Initiated Buprenorphine for Opioid Use Disorder.Ann Emerg Med. 2025 Mar;85(3):205-213. doi: 10.1016/j.annemergmed.2024.10.001. Epub 2024 Nov 20. Ann Emerg Med. 2025. PMID: 39570250
References
-
- Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2016 (GBD 2016) data resources. 2017. Accessed at http://ghdx.healthdata.org/gbd-2016 on 12 November 2017.
-
- Gruber SA, Silveri MM, Yurgelun-Todd DA. Neuropsychological consequences of opiate use. Neuropsychol Rev. 2007;17:299–315. [PMID: ] - PubMed
-
- Manchikanti L, Fellows B, Ailinani H, Pampati V. Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. Pain Physician. 2010;13:401–35. [PMID: ] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 DA013046/DA/NIDA NIH HHS/United States
- U10 DA015831/DA/NIDA NIH HHS/United States
- U10 DA013035/DA/NIDA NIH HHS/United States
- UG1 DA013034/DA/NIDA NIH HHS/United States
- UG1 DA013720/DA/NIDA NIH HHS/United States
- HHSN271201200017C/DA/NIDA NIH HHS/United States
- P30 DA040500/DA/NIDA NIH HHS/United States
- R01 DA035808/DA/NIDA NIH HHS/United States
- UG1 DA013714/DA/NIDA NIH HHS/United States
- U10 DA013714/DA/NIDA NIH HHS/United States
- UG1 DA015831/DA/NIDA NIH HHS/United States
- UG1 DA013035/DA/NIDA NIH HHS/United States
- HHSN271201500065C/DA/NIDA NIH HHS/United States
- U10 DA013732/DA/NIDA NIH HHS/United States
- K24 DA022412/DA/NIDA NIH HHS/United States
- U10 DA013045/DA/NIDA NIH HHS/United States
- U10 DA013034/DA/NIDA NIH HHS/United States
- UG1 DA013732/DA/NIDA NIH HHS/United States
- U10 DA015833/DA/NIDA NIH HHS/United States
- U10 DA013720/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials