

Validation of Diagnostic and Performance Characteristics of the Wireless Motility Capsule in Patients With Suspected Gastroparesis
- PMID: 30557741
- PMCID: PMC7442471
- DOI: 10.1016/j.cgh.2018.11.063
Validation of Diagnostic and Performance Characteristics of the Wireless Motility Capsule in Patients With Suspected Gastroparesis
Abstract
Background & aims: It is a challenge to make a diagnosis of gastroparesis. There is good agreement in results from wireless motility capsule (WMC) analysis and gastric emptying scintigraphy (GES), but the diagnostic yield of WMC is unclear and the accuracy of this method has not been validated. We compared the performance characteristics of WMC vs GES in assessing gastric emptying in patients with suspected gastroparesis.
Methods: We performed a prospective study of 167 subjects with gastroparesis (53 with diabetes and 114 without) at 10 centers, from 2013 through 2016. Subjects were assessed simultaneously by GES and with a WMC to measure gastric emptying and regional transit. Delayed gastric emptying by GES was defined as more than 10% meal retention at 4 hrs whereas delayed gastric emptying by WMC was defined as more than 5 hrs for passage of the capsule into the duodenum; a severe delay in gastric emptying was defined as a gastric emptying time of more than 12 hrs by WMC or more than 35% retention at 4 hrs by GES. Rapid gastric emptying was defined as less than 38% meal retention at 1 hr based on by GES or gastric emptying times less than 1:45 hrs by WMC. We compared diagnostic and performance characteristics of GES vs WMC.
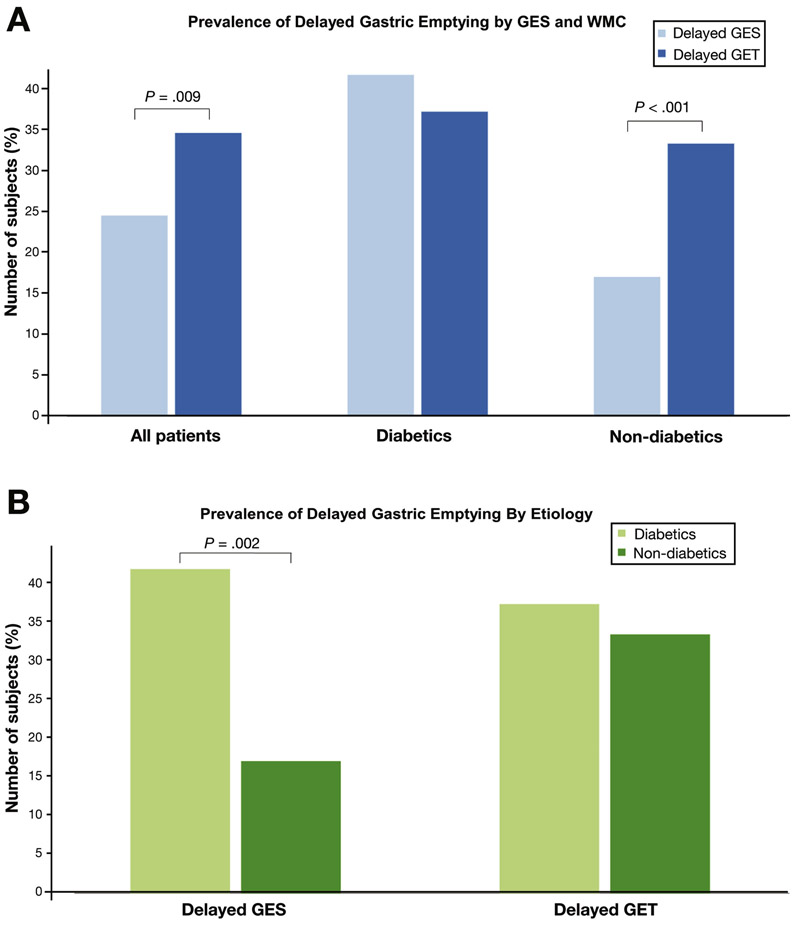
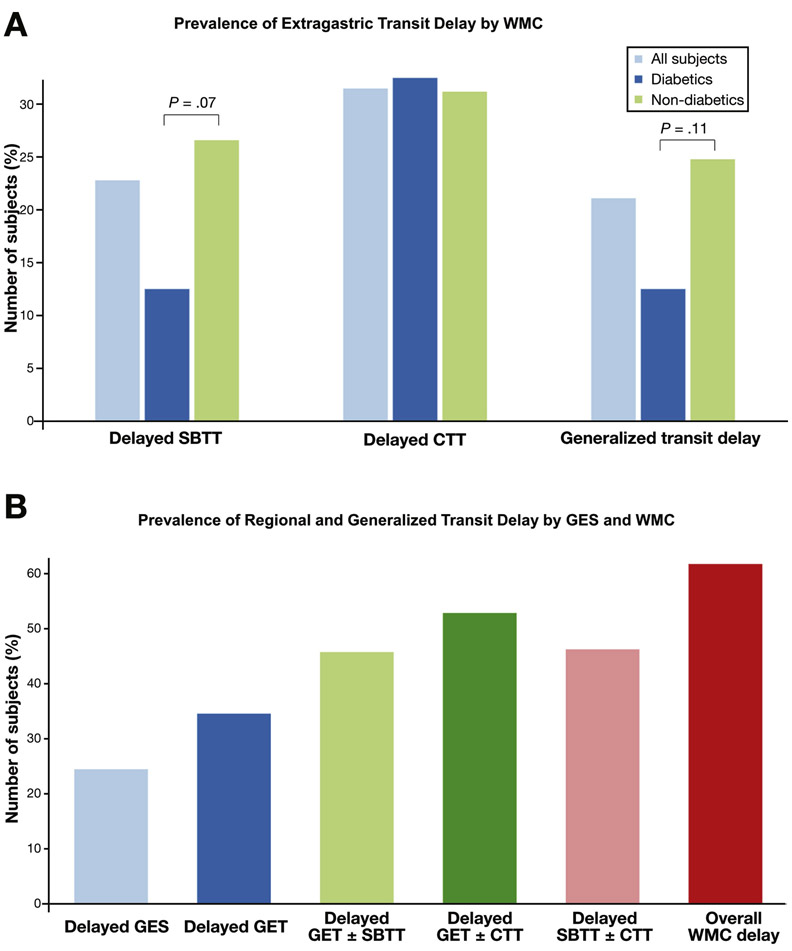
Results: Delayed gastric emptying was detected in a higher proportion of subjects by WMC (34.6%) than by GES (24.5%) (P=.009). Overall agreement in results between methods was 75.7% (kappa=0.42). In subjects without diabetes, the WMC detected a higher proportion of subjects with delayed gastric emptying (33.3%) than GES (17.1%) (P < .001). A higher proportion of subjects with diabetes had delayed gastric emptying detected by GES (41.7%) compared with non-diabetic subjects (17.1%) (P=.002). Severe delays in gastric emptying were observed in a higher proportion of subjects by WMC (13.8%) than by GES (6.9%) (P = .02). Rapid gastric emptying was detected in a higher proportion of subjects by GES (13.8%) than by WMC (3.3%) (P < .001). Regional and generalized transit abnormalities were observed in 61.8% subjects and only detected by WMC.
Conclusion: Although there is agreement in analysis of gastric emptying by GES vs WMC, WMC provides higher diagnostic yield than GES. WMC detects delayed gastric emptying more frequently than GES and identifies extra-gastric transit abnormalities. Diabetic vs non-diabetic subjects have different results from GES vs WMC. These findings could affect management of patients with suspected gastroparesis. ClinicalTrials.gov no: NCT02022826.
Keywords: Colonic Transit; Gastrointestinal Motility; Idiopathic; Small Bowel Transit.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Murky Waters for Diagnosis of Gastroparesis.Clin Gastroenterol Hepatol. 2019 Aug;17(9):1724-1725. doi: 10.1016/j.cgh.2019.04.008. Epub 2019 Apr 9. Clin Gastroenterol Hepatol. 2019. PMID: 30978538 No abstract available.
References
-
- Abell TL, Camilleri M, Donohoe K, et al. Consensus Recommendations for Gastric Emptying Scintigraphy: A Joint Report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am J Gastroenterol 2008;103:753–763. - PubMed
-
- Rao SSC, Mysore K, Attaluri A, et al. Diagnostic utility of wireless motility capsule in gastrointestinal dysmotility. J Clin Gastroenterol 2011;45:684–690. - PubMed
-
- Kuo B, Maneerattanaporn M, Lee AA, et al. Generalized transit delay on wireless motility capsule testing in patients with clinical suspicion of gastroparesis, small intestinal dysmotility, or slow transit constipation. Dig Dis Sci 2011;56:2928–2938. - PubMed
-
- Kuo B, McCallum RW, Koch KL, et al. Comparison of gastric emptying of a nondigestible capsule to a radio-labelled meal in healthy and gastroparetic subjects. Aliment Pharmacol Ther 2008;27:186–196. - PubMed
