

Do Androgens Modulate the Pathophysiological Pathways of Inflammation? Appraising the Contemporary Evidence
- PMID: 30558178
- PMCID: PMC6306858
- DOI: 10.3390/jcm7120549
Do Androgens Modulate the Pathophysiological Pathways of Inflammation? Appraising the Contemporary Evidence
Abstract
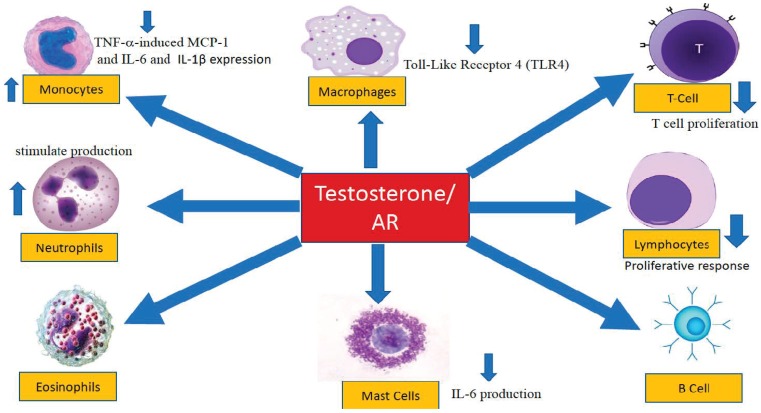
The role of testosterone in the pathophysiology of inflammation is of critical clinical importance; however, no universal mechanism(s) has been advanced to explain the complex and interwoven pathways of androgens in the attenuation of the inflammatory processes. PubMed and EMBASE searches were performed, including the following key words: "testosterone", "androgens", "inflammatory cytokines", "inflammatory biomarkers" with focus on clinical studies as well as basic scientific studies in human and animal models. Significant benefits of testosterone therapy in ameliorating or attenuating the symptoms of several chronic inflammatory diseases were reported. Because anti⁻tumor necrosis factor therapy is the mainstay for the treatment of moderate-to-severe inflammatory bowel disease; including Crohn's disease and ulcerative colitis, and because testosterone therapy in hypogonadal men with chronic inflammatory conditions reduce tumor necrosis factor-alpha (TNF-α), IL-1β, and IL-6, we suggest that testosterone therapy attenuates the inflammatory process and reduces the burden of disease by mechanisms inhibiting inflammatory cytokine expression and function. Mechanistically, androgens regulate the expression and function of inflammatory cytokines, including TNF-α, IL-1β, IL-6, and CRP (C-reactive protein). Here, we suggest that testosterone regulates multiple and overlapping cellular and molecular pathways involving a host of immune cells and biochemical factors that converge to contribute to attenuation of the inflammatory process.
Keywords: C-reactive protein; chronic inflammatory diseases; interleukin-1 beta; interleukin-6; testosterone; tumor necrosis factor-alpha.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Enhanced secretion of tumour necrosis factor-alpha, IL-6, and IL-1 beta by isolated lamina propria mononuclear cells from patients with ulcerative colitis and Crohn's disease.Clin Exp Immunol. 1993 Oct;94(1):174-81. doi: 10.1111/j.1365-2249.1993.tb05997.x. Clin Exp Immunol. 1993. PMID: 8403503 Free PMC article.
-
KFL2 participates in the development of ulcerative colitis through inhibiting inflammation via regulating cytokines.Eur Rev Med Pharmacol Sci. 2018 Aug;22(15):4941-4948. doi: 10.26355/eurrev_201808_15633. Eur Rev Med Pharmacol Sci. 2018. PMID: 30070340
-
The protease inhibitor cystatin C down-regulates the release of IL-β and TNF-α in lipopolysaccharide activated monocytes.J Leukoc Biol. 2016 Oct;100(4):811-822. doi: 10.1189/jlb.5A0415-174R. Epub 2016 May 17. J Leukoc Biol. 2016. PMID: 27190304
-
The relationship between circulating testosterone and inflammatory cytokines in men.Aging Male. 2019 Jun;22(2):129-140. doi: 10.1080/13685538.2018.1482487. Epub 2018 Jun 21. Aging Male. 2019. PMID: 29925283 Review.
-
Cytokines, acute-phase proteins, and hormones: IL-1 and TNF-alpha production in contact-mediated activation of monocytes by T lymphocytes.Ann N Y Acad Sci. 2002 Jun;966:464-73. doi: 10.1111/j.1749-6632.2002.tb04248.x. Ann N Y Acad Sci. 2002. PMID: 12114305 Review.
Cited by
-
H7N9 avian influenza virus infection in men is associated with testosterone depletion.Nat Commun. 2022 Nov 14;13(1):6936. doi: 10.1038/s41467-022-34500-5. Nat Commun. 2022. PMID: 36376288 Free PMC article.
-
Oat Beta-Glucan Dietary Intervention on Antioxidant Defense Parameters, Inflammatory Response and Angiotensin Signaling in the Testes of Rats with TNBS-Induced Colitis.Nutrients. 2024 Aug 3;16(15):2546. doi: 10.3390/nu16152546. Nutrients. 2024. PMID: 39125425 Free PMC article.
-
Recent Update on the Molecular Mechanisms of Gonadal Steroids Action in Adipose Tissue.Int J Mol Sci. 2021 May 14;22(10):5226. doi: 10.3390/ijms22105226. Int J Mol Sci. 2021. PMID: 34069293 Free PMC article. Review.
-
Androgen Exhibits a Protective Role Against Focal Erosions in Murine TNF-induced Inflammatory Arthritis.J Endocr Soc. 2024 Oct 1;8(11):bvae169. doi: 10.1210/jendso/bvae169. eCollection 2024 Sep 26. J Endocr Soc. 2024. PMID: 39416428 Free PMC article.
-
Sex Hormones and Novel Corona Virus Infectious Disease (COVID-19).Mayo Clin Proc. 2020 Aug;95(8):1710-1714. doi: 10.1016/j.mayocp.2020.05.013. Epub 2020 May 29. Mayo Clin Proc. 2020. PMID: 32753145 Free PMC article. Review.
References
-
- Ashley N.T., Weil Z.M., Nelson R.J. Inflammation: Mechanisms, Costs, and Natural Variation. Annu. Rev. Ecol. Evol. Syst. 2012;43:385–406. doi: 10.1146/annurev-ecolsys-040212-092530. - DOI
-
- Miligkos M., Papamichael K., Vande Casteele N., Mantzaris G.J., Giles A., Levesque B.G., Zintzaras E. Efficacy and safety profile of anti-tumor necrosis factor-α versus anti-integrin agents for the treatment of Crohn’s disease: A network meta-analysis of indirect comparisons. Clin. Ther. 2016;38:1342–1358. doi: 10.1016/j.clinthera.2016.03.018. - DOI - PubMed
-
- Choy E.H., Bernasconi C., Aassi M., Molina J.F., Epis O.M. Treatment of Rheumatoid Arthritis With Anti–Tumor Necrosis Factor or Tocilizumab Therapy as First Biologic Agent in a Global Comparative Observational Study. Arthritis Care Res. 2017;69:1484–1494. doi: 10.1002/acr.23303. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
