

Executive Summary of Stroke Statistics in Korea 2018: A Report from the Epidemiology Research Council of the Korean Stroke Society
- PMID: 30558400
- PMCID: PMC6372894
- DOI: 10.5853/jos.2018.03125
Executive Summary of Stroke Statistics in Korea 2018: A Report from the Epidemiology Research Council of the Korean Stroke Society
Abstract
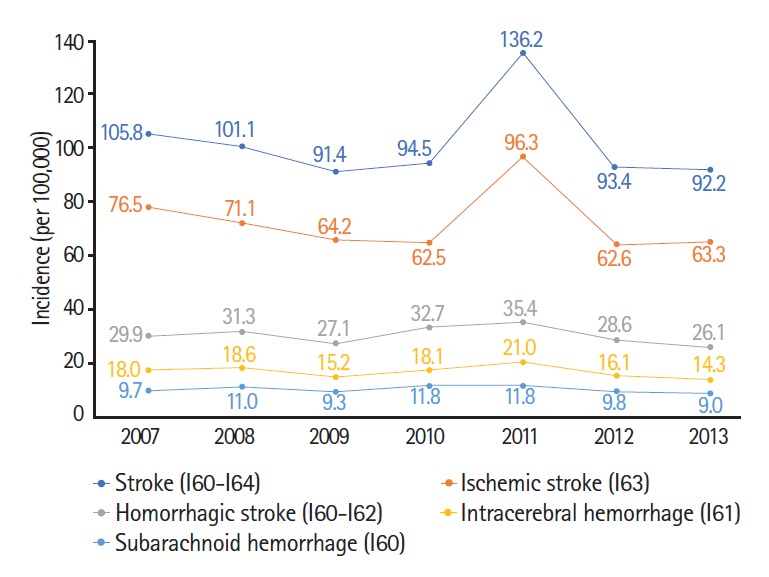
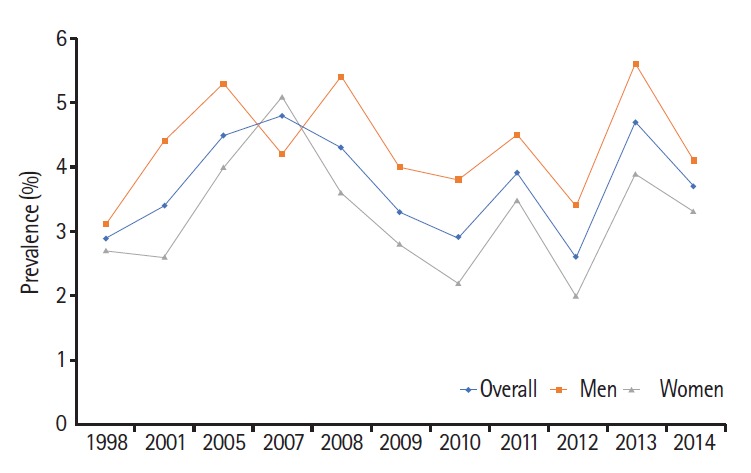
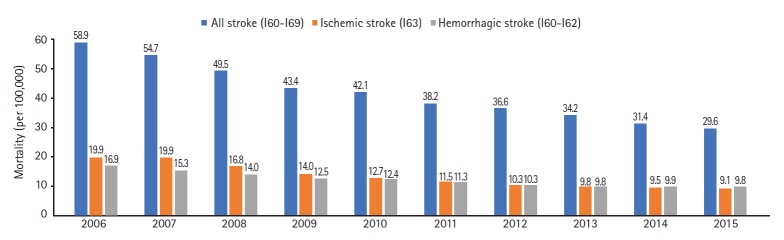
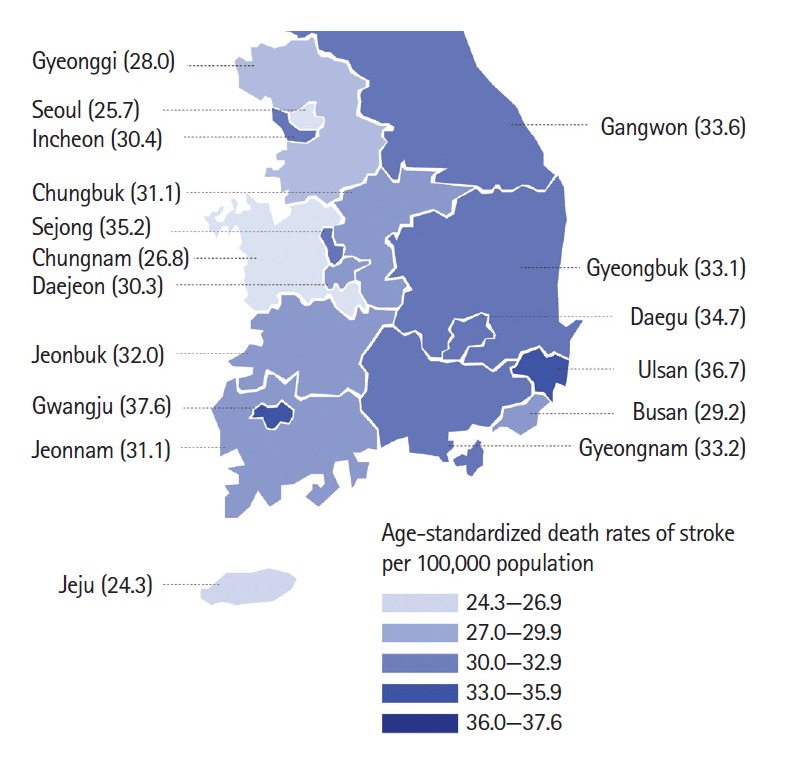
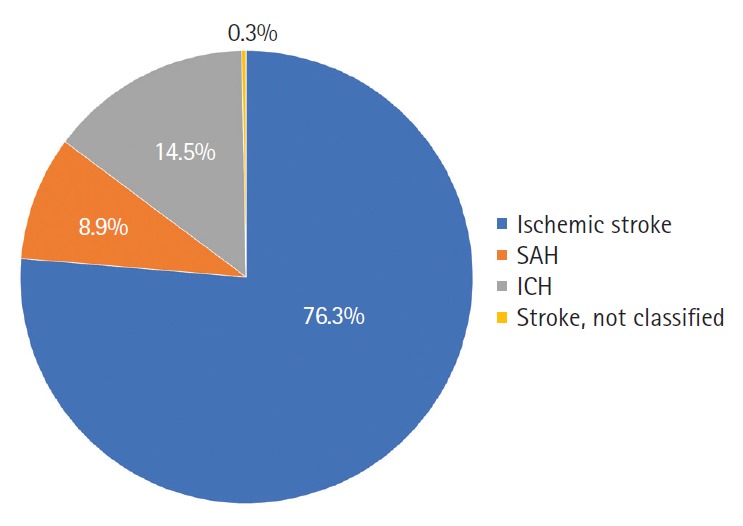
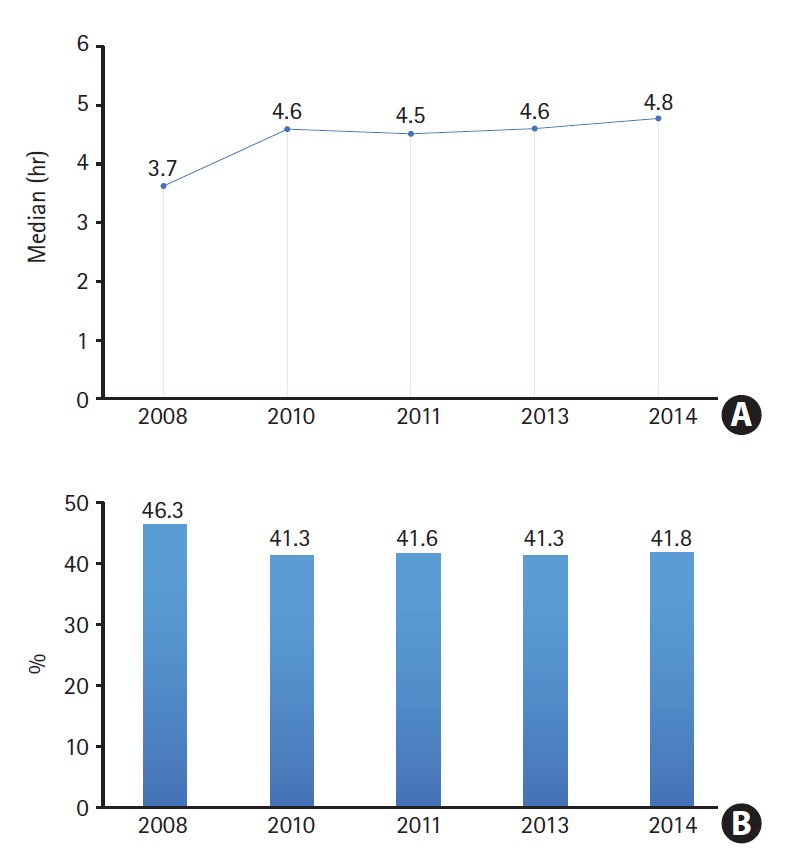
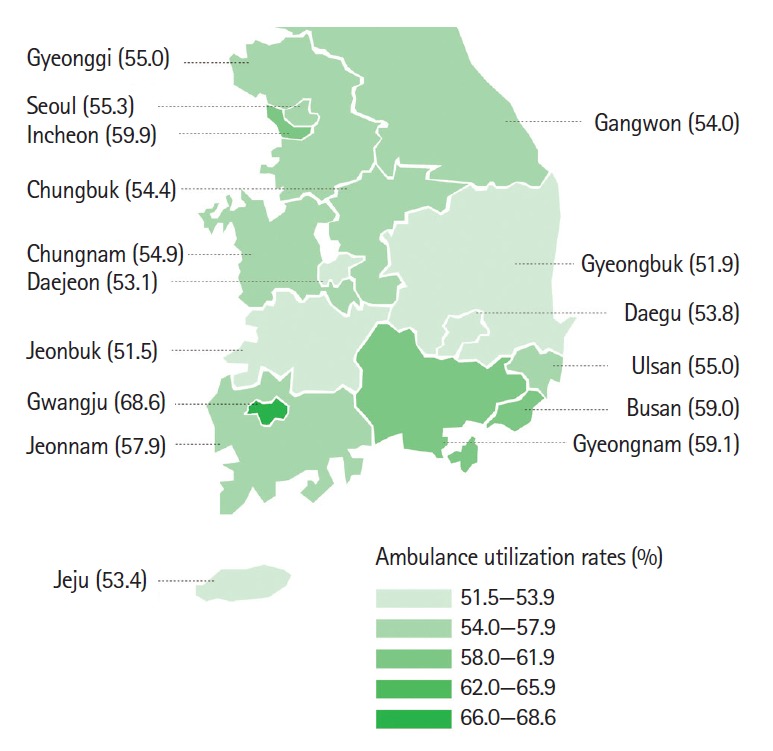
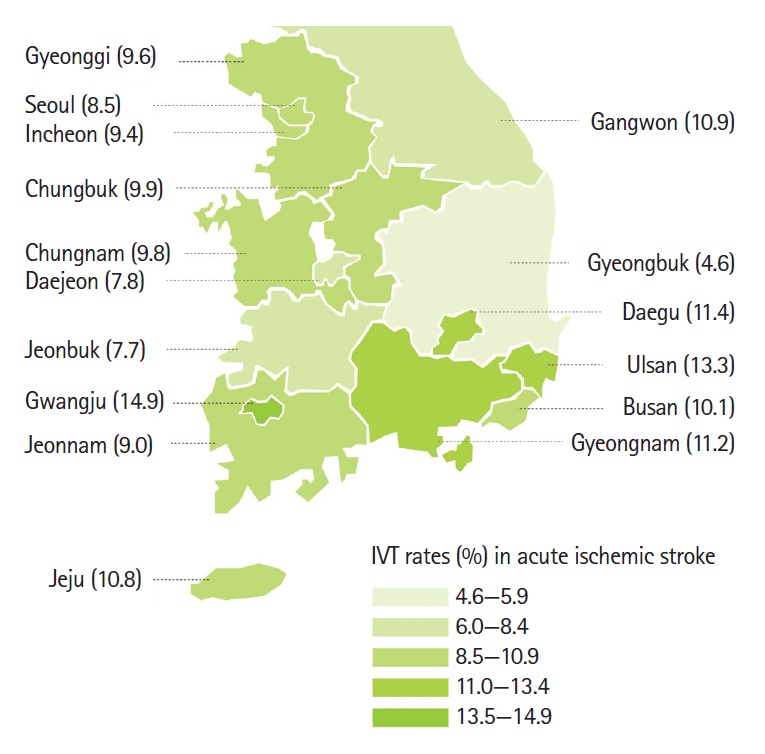
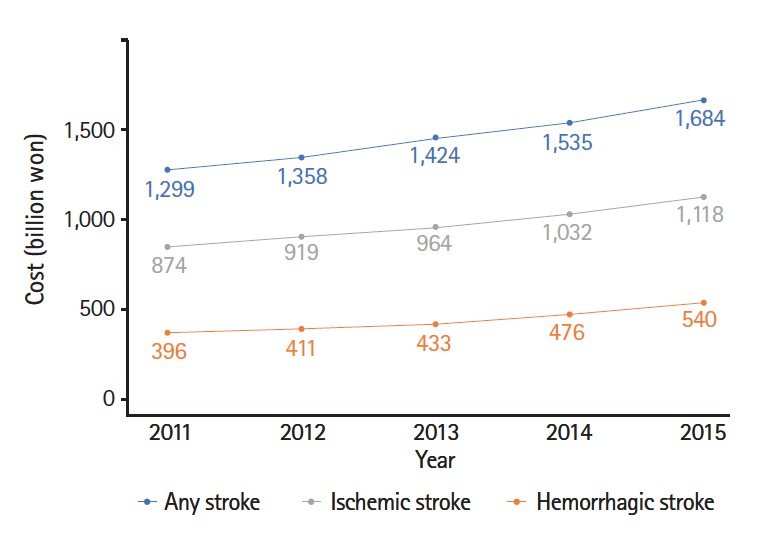
Despite the great socioeconomic burden of stroke, there have been few reports of stroke statistics in Korea. In this scenario, the Epidemiologic Research Council of the Korean Stroke Society launched the "Stroke Statistics in Korea" project, aimed at writing a contemporary, comprehensive, and representative report on stroke epidemiology in Korea. This report contains general statistics of stroke, prevalence of behavioral and vascular risk factors, stroke characteristics, pre-hospital system of care, hospital management, quality of stroke care, and outcomes. In this report, we analyzed the most up-to-date and nationally representative databases, rather than performing a systematic review of existing evidence. In summary, one in 40 adults are patients with stroke and 232 subjects per 100,000 experience a stroke event every year. Among the 100 patients with stroke in 2014, 76 had ischemic stroke, 15 had intracerebral hemorrhage, and nine had subarachnoid hemorrhage. Stroke mortality is gradually declining, but it remains as high as 30 deaths per 100,000 individuals, with regional disparities. As for stroke risk factors, the prevalence of smoking is decreasing in men but not in women, and the prevalence of alcohol drinking is increasing in women but not in men. Population-attributable risk factors vary with age. Smoking plays a role in young-aged individuals, hypertension and diabetes in middle-aged individuals, and atrial fibrillation in the elderly. About four out of 10 hospitalized patients with stroke are visiting an emergency room within 3 hours of symptom onset, and only half use an ambulance. Regarding acute management, the proportion of patients with ischemic stroke receiving intravenous thrombolysis and endovascular treatment was 10.7% and 3.6%, respectively. Decompressive surgery was performed in 1.4% of patients with ischemic stroke and in 28.1% of those with intracerebral hemorrhage. The cumulative incidence of bleeding and fracture at 1 year after stroke was 8.9% and 4.7%, respectively. The direct costs of stroke were about ₩1.68 trillion (KRW), of which ₩1.11 trillion were for ischemic stroke and ₩540 billion for hemorrhagic stroke. The great burden of stroke in Korea can be reduced through more concentrated efforts to control major attributable risk factors for age and sex, reorganize emergency medical service systems to give patients with stroke more opportunities for reperfusion therapy, disseminate stroke unit care, and reduce regional disparities. We hope that this report can contribute to achieving these tasks.
Keywords: Epidemiology; Statistics; Stroke.
Figures

References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223. - PubMed
-
- Korean Statistical Information Service (KOSIS) Annual Report on the Causes of Death Statistics. Daejeon: Statistics Korea; 2016.
-
- Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
