

Pilot study of decision support tools on breast cancer chemoprevention for high-risk women and healthcare providers in the primary care setting
- PMID: 30558581
- PMCID: PMC6296071
- DOI: 10.1186/s12911-018-0716-5
Pilot study of decision support tools on breast cancer chemoprevention for high-risk women and healthcare providers in the primary care setting
Abstract
Background: Breast cancer chemoprevention can reduce breast cancer incidence in high-risk women; however, chemoprevention is underutilized in the primary care setting. We conducted a pilot study of decision support tools among high-risk women and their primary care providers (PCPs).
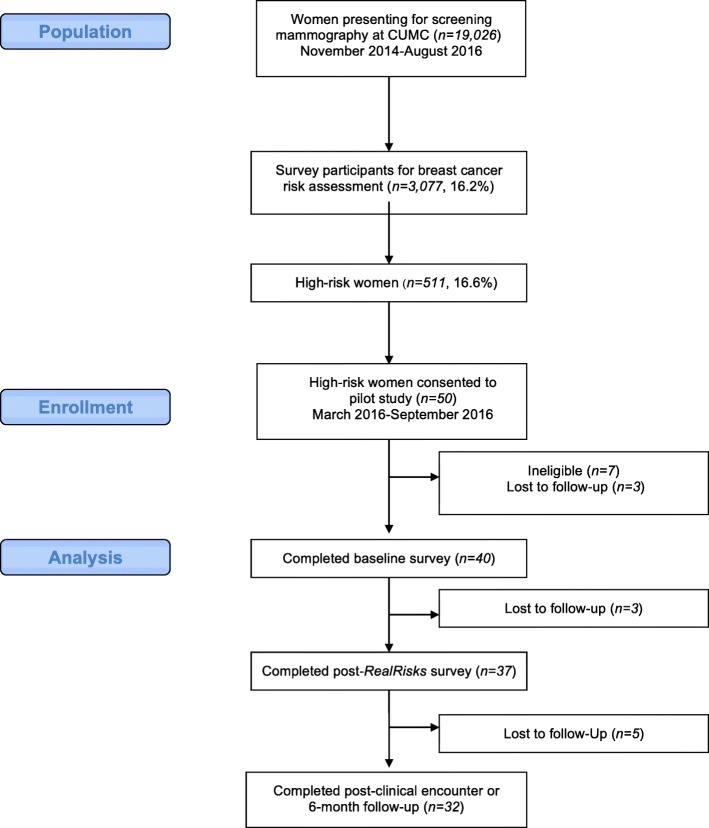
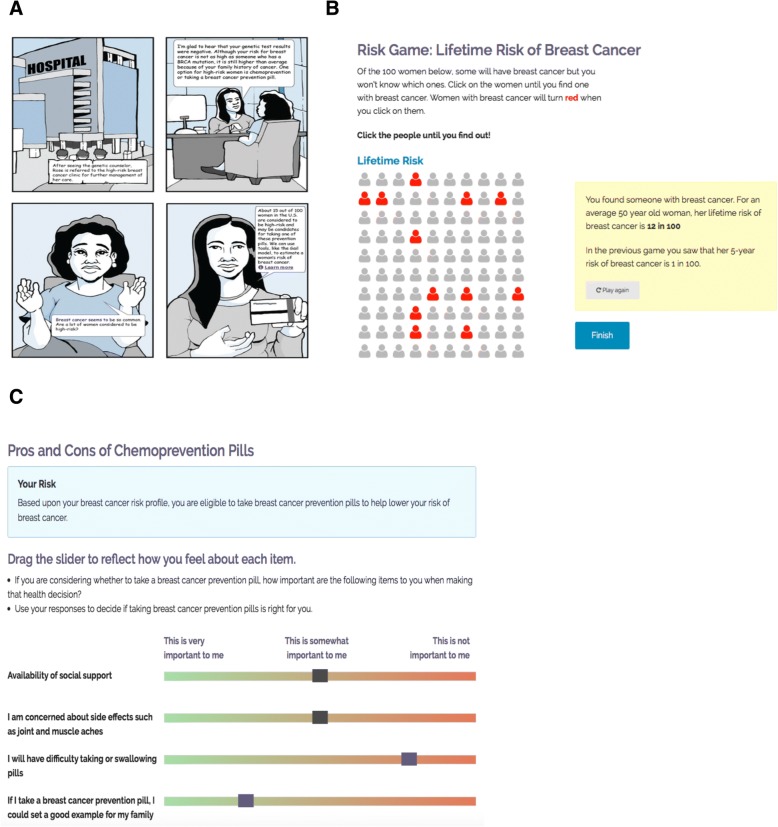
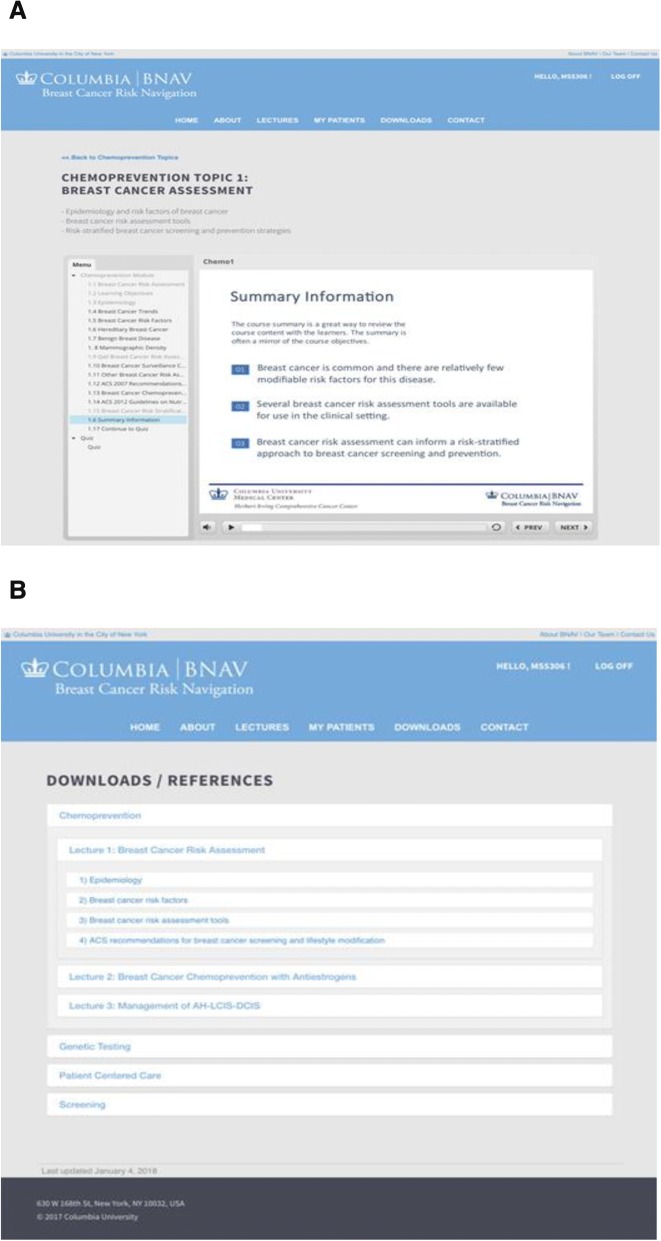
Methods: The intervention included a decision aid (DA) for high-risk women, RealRisks, and a provider-centered tool, Breast Cancer Risk Navigation (BNAV). Patients completed validated surveys at baseline, after RealRisks and after their PCP clinical encounter or at 6-months. Referral for high-risk consultation and chemoprevention uptake were assessed via the electronic health record. The primary endpoint was accuracy of breast cancer risk perception at 6-months.
Results: Among 40 evaluable high-risk women, median age was 64.5 years and median 5-year breast cancer risk was 2.19%. After exposure to RealRisks, patients demonstrated an improvement in accurate breast cancer risk perceptions (p = 0.02), an increase in chemoprevention knowledge (p < 0.01), and 24% expressed interest in taking chemoprevention. Three women had a high-risk referral, and no one initiated chemoprevention. Decisional conflict significantly increased from after exposure to RealRisks to after their clinical encounter or at 6-months (p < 0.01). Accurate breast cancer risk perceptions improved and was sustained at 6-months or after clinical encounters. We discuss the side effect profile of chemoprevention and the care pathway when RealRisks was introduced to understand why patients experienced increased decision conflict.
Conclusion: Future interventions should carefully link the use of a DA more proximally to the clinical encounter, investigate timed measurements of decision conflict and improve risk communication, shared decision making, and chemoprevention education for PCPs. Additional work remains to better understand the impact of decision aids targeting both patients and providers.
Trial registration: ClinicalTrials.gov Identifier: NCT02954900 November 4, 2016 Retrospectively registered.
Keywords: Breast cancer; Chemoprevention; Decision aids; Decision conflict; Decision support; Risk communication.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Columbia University, IRB AAAP4151. Informed consent was obtained from all individual participants included in the study. Consent to participate was given in written form. All procedures performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Qualitative analysis of shared decision-making for chemoprevention in the primary care setting: provider-related barriers.BMC Med Inform Decis Mak. 2022 Aug 4;22(1):208. doi: 10.1186/s12911-022-01954-y. BMC Med Inform Decis Mak. 2022. PMID: 35927732 Free PMC article. Clinical Trial.
-
Perceptions of Racially and Ethnically Diverse Women at High Risk of Breast Cancer Regarding the Use of a Web-Based Decision Aid for Chemoprevention: Qualitative Study Nested Within a Randomized Controlled Trial.J Med Internet Res. 2021 Jun 8;23(6):e23839. doi: 10.2196/23839. J Med Internet Res. 2021. PMID: 34100769 Free PMC article. Clinical Trial.
-
Study protocol: a cluster randomized controlled trial of web-based decision support tools for increasing BRCA1/2 genetic counseling referral in primary care.BMC Health Serv Res. 2018 Aug 13;18(1):633. doi: 10.1186/s12913-018-3442-x. BMC Health Serv Res. 2018. PMID: 30103738 Free PMC article. Clinical Trial.
-
Communicating prognosis to women with early breast cancer - overview of prediction tools and the development and pilot testing of a decision aid.BMC Health Serv Res. 2019 Mar 15;19(1):171. doi: 10.1186/s12913-019-3988-2. BMC Health Serv Res. 2019. PMID: 30876414 Free PMC article.
-
Effectiveness of decision aids for female BRCA1 and BRCA2 mutation carriers: a systematic review.BMC Med Inform Decis Mak. 2019 Aug 1;19(1):154. doi: 10.1186/s12911-019-0872-2. BMC Med Inform Decis Mak. 2019. PMID: 31370837 Free PMC article.
Cited by
-
Qualitative analysis of shared decision-making for chemoprevention in the primary care setting: provider-related barriers.BMC Med Inform Decis Mak. 2022 Aug 4;22(1):208. doi: 10.1186/s12911-022-01954-y. BMC Med Inform Decis Mak. 2022. PMID: 35927732 Free PMC article. Clinical Trial.
-
Patient and Clinician Decision Support to Increase Genetic Counseling for Hereditary Breast and Ovarian Cancer Syndrome in Primary Care: A Cluster Randomized Clinical Trial.JAMA Netw Open. 2022 Jul 1;5(7):e2222092. doi: 10.1001/jamanetworkopen.2022.22092. JAMA Netw Open. 2022. PMID: 35849397 Free PMC article. Clinical Trial.
-
Use of web-based decision support to improve informed choice for chemoprevention: a qualitative analysis of pre-implementation interviews (SWOG S1904).BMC Med Inform Decis Mak. 2024 Sep 27;24(1):272. doi: 10.1186/s12911-024-02691-0. BMC Med Inform Decis Mak. 2024. PMID: 39334347 Free PMC article. Clinical Trial.
-
User Comprehension and EHR Integration of the RealRisks Decision Aid for Breast Cancer Risk Assessment: A Qualitative Study.AMIA Annu Symp Proc. 2025 May 22;2024:1129-1138. eCollection 2024. AMIA Annu Symp Proc. 2025. PMID: 40417528 Free PMC article.
-
Knowledge of Potential Harms and Benefits of Tamoxifen among Women Considering Breast Cancer Preventive Therapy.Cancer Prev Res (Phila). 2020 Apr;13(4):411-422. doi: 10.1158/1940-6207.CAPR-19-0424. Epub 2020 Jan 27. Cancer Prev Res (Phila). 2020. PMID: 31988145 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. - PubMed
-
- American Cancer Society. Cancer Facts & Figures 2017. 2017; https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts....
-
- Costantino JP, Gail MH, Pee D, et al. Validation studies for models projecting the risk of invasive and total breast cancer incidence. J Natl Cancer Inst. 1999;91(18):1541–1548. - PubMed
-
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and bowel project P-1 study. J Natl Cancer Inst. 2005;97(22):1652–1662. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
