

Tigecycline in critically ill patients on continuous renal replacement therapy: a population pharmacokinetic study
- PMID: 30558639
- PMCID: PMC6296114
- DOI: 10.1186/s13054-018-2278-4
Tigecycline in critically ill patients on continuous renal replacement therapy: a population pharmacokinetic study
Abstract
Background: Tigecycline is a vital antibiotic treatment option for infections caused by multiresistant bacteria in the intensive care unit (ICU). Acute kidney injury (AKI) is a common complication in the ICU requiring continuous renal replacement therapy (CRRT), but pharmacokinetic data for tigecycline in patients receiving CRRT are lacking.
Methods: Eleven patients mainly with intra-abdominal infections receiving either continuous veno-venous hemodialysis (CVVHD, n = 8) or hemodiafiltration (CVVHDF, n = 3) were enrolled, and plasma as well as effluent samples were collected according to a rich sampling schedule. Total and free tigecycline was determined by ultrafiltration and high-performance liquid chromatography (HPLC)-UV. Population pharmacokinetic modeling using NONMEM® 7.4 was used to determine the pharmacokinetic parameters as well as the clearance of CVVHD and CVVHDF. Pharmacokinetic/pharmacodynamic target attainment analyses were performed to explore the potential need for dose adjustments of tigecycline in CRRT.
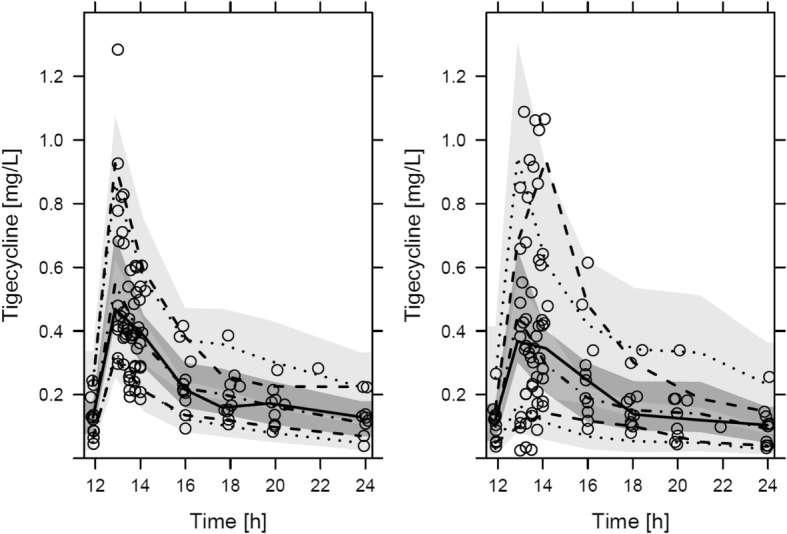
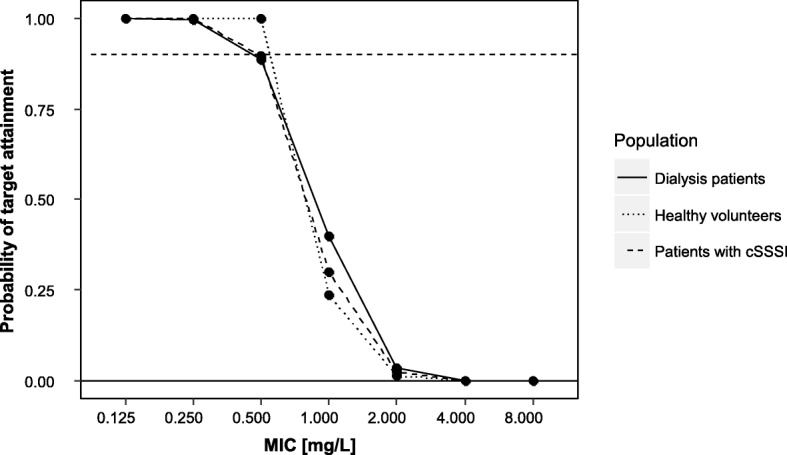
Results: A two-compartment population pharmacokinetic (PK) model was suitable to simultaneously describe the plasma PK and effluent measurements of tigecycline. Tigecycline dialysability was high, as indicated by the high mean saturation coefficients of 0.79 and 0.90 for CVVHD and CVVHDF, respectively, and in range of the concentration-dependent unbound fraction of tigecycline (45-94%). However, the contribution of CRRT to tigecycline clearance (CL) was only moderate (CLCVVHD: 1.69 L/h, CLCVVHDF: 2.71 L/h) in comparison with CLbody (physiological part of the total clearance) of 18.3 L/h. Bilirubin was identified as a covariate on CLbody in our collective, reducing the observed interindividual variability on CLbody from 58.6% to 43.6%. The probability of target attainment under CRRT for abdominal infections was ≥ 0.88 for minimal inhibitory concentration (MIC) values ≤ 0.5 mg/L and similar to patients without AKI.
Conclusions: Despite high dialysability, dialysis clearance displayed only a minor contribution to tigecycline elimination, being in the range of renal elimination in patients without AKI. No dose adjustment of tigecycline seems necessary in CRRT.
Trial registration: EudraCT, 2012-005617-39 . Registered on 7 August 2013.
Keywords: CVVHD; CVVHDF; Dosing; NONMEM; Population pharmacokinetics; Renal replacement therapy; Tigecycline.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the ethics committee at the medical faculty of the University of Tübingen (no. 057/2013AMG1) and the German Federal Institute for Drugs and Medical Devices (Eudra-CT number 2012–005617-39).
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
No dose adjustment of tigecycline is necessary during continuous renal replacement therapy: we are not sure.Crit Care. 2020 Feb 20;24(1):59. doi: 10.1186/s13054-020-2775-0. Crit Care. 2020. PMID: 32079536 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
