

Why the evolution of vaccine resistance is less of a concern than the evolution of drug resistance
- PMID: 30559199
- PMCID: PMC6304978
- DOI: 10.1073/pnas.1717159115
Why the evolution of vaccine resistance is less of a concern than the evolution of drug resistance
Abstract
Vaccines and antimicrobial drugs both impose strong selection for resistance. Yet only drug resistance is a major challenge for 21st century medicine. Why is drug resistance ubiquitous and not vaccine resistance? Part of the answer is that vaccine resistance is far less likely to evolve than drug resistance. But what happens when vaccine resistance does evolve? We review six putative cases. We find that in contrast to drug resistance, vaccine resistance is harder to detect and harder to confirm and that the mechanistic basis is less well understood. Nevertheless, in the cases we examined, the pronounced health benefits associated with vaccination have largely been sustained. Thus, we contend that vaccine resistance is less of a concern than drug resistance because it is less likely to evolve and when it does, it is less harmful to human and animal health and well-being. Studies of pathogen strains that evolve the capacity to replicate and transmit from vaccinated hosts will enhance our ability to develop next-generation vaccines that minimize the risk of harmful pathogen evolution.
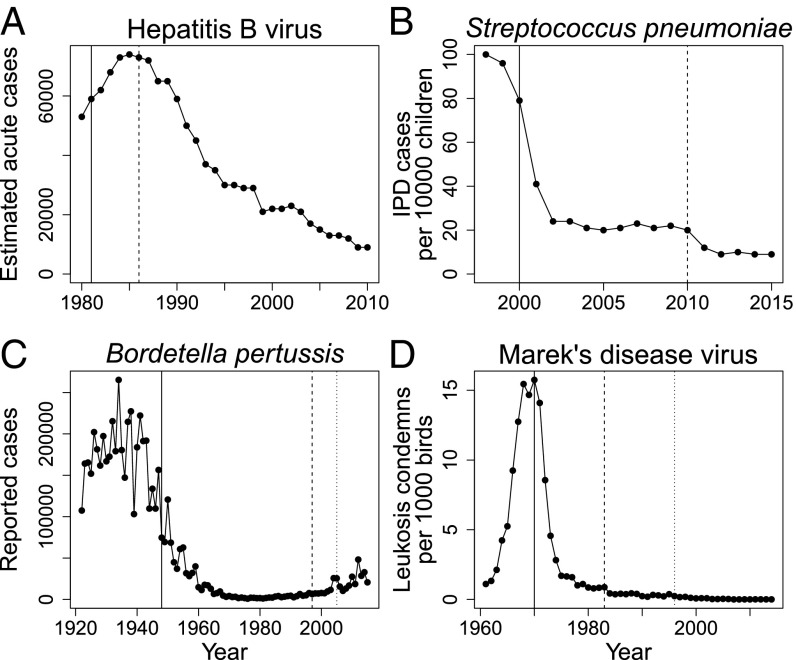
Keywords: HBV; Marek’s disease virus; Streptococcus; evolutionary rescue; pertussis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Why does drug resistance readily evolve but vaccine resistance does not?Proc Biol Sci. 2017 Mar 29;284(1851):20162562. doi: 10.1098/rspb.2016.2562. Proc Biol Sci. 2017. PMID: 28356449 Free PMC article. Review.
-
The Influence of Major Histocompatibility Complex and Vaccination with Turkey Herpesvirus on Marek's Disease Virus Evolution.Avian Dis. 2015 Mar;59(1):122-9. doi: 10.1637/10677-092413-reg. Avian Dis. 2015. PMID: 26292545
-
A Chinese Variant Marek's Disease Virus Strain with Divergence between Virulence and Vaccine Resistance.Viruses. 2017 Apr 3;9(4):71. doi: 10.3390/v9040071. Viruses. 2017. PMID: 28368367 Free PMC article.
-
Molecular evaluation of responses to vaccination and challenge by Marek's disease viruses.Avian Pathol. 2007 Oct;36(5):351-9. doi: 10.1080/03079450701557149. Avian Pathol. 2007. PMID: 17899458 Clinical Trial.
-
Vaccinal control of Marek's disease: current challenges, and future strategies to maximize protection.Vet Immunol Immunopathol. 2006 Jul 15;112(1-2):78-86. doi: 10.1016/j.vetimm.2006.03.014. Epub 2006 May 8. Vet Immunol Immunopathol. 2006. PMID: 16682084 Review.
Cited by
-
Differences in Pathogenicity and Vaccine Resistance Discovered between Two Epidemic Strains of Marek's Disease Virus in China.Viruses. 2023 Apr 11;15(4):945. doi: 10.3390/v15040945. Viruses. 2023. PMID: 37112925 Free PMC article.
-
Prediction of Burkholderia pseudomallei DsbA substrates identifies potential virulence factors and vaccine targets.PLoS One. 2020 Nov 20;15(11):e0241306. doi: 10.1371/journal.pone.0241306. eCollection 2020. PLoS One. 2020. PMID: 33216758 Free PMC article.
-
Enhancing vaccine effectiveness in the elderly to counter antibiotic resistance: The potential of adjuvants via pattern recognition receptors.Hum Vaccin Immunother. 2024 Dec 31;20(1):2317439. doi: 10.1080/21645515.2024.2317439. Epub 2024 Mar 4. Hum Vaccin Immunother. 2024. PMID: 39693178 Free PMC article. Review.
-
Vaccine impact on antimicrobial resistance to inform Gavi, the Vaccine Alliance's 2018 Vaccine Investment Strategy: report from an expert survey.F1000Res. 2019 Sep 24;8:1685. doi: 10.12688/f1000research.20100.1. eCollection 2019. F1000Res. 2019. PMID: 31737260 Free PMC article.
-
Lipopeptide adjuvants for antibiotics and vaccines: the future step in the fight against multidrug-resistant and extensively drug-resistant pathogens.Explor Drug Sci. 2024;2:203-233. doi: 10.37349/eds.2024.00043. Epub 2024 Apr 29. Explor Drug Sci. 2024. PMID: 40842601 Free PMC article.
References
-
- Arias E, Heron M, Xu J. Division of Vital Statistics . United States Life Tables, 2012. Vol 65. US Department of Health and Human Services, Centers for Disease Control and Prevention; and Prevention; Hyattsville, MD: 2016. pp. 46–47. - PubMed
-
- Cromwell GL. Why and how antibiotics are used in swine production. Anim Biotechnol. 2002;13:7–27. - PubMed
-
- Morrow C, Fehler F. Marek’s disease: A worldwide problem. In: Davison F, Nair V, editors. Marek’s Disease: An Evolving Problem. Elsevier; San Diego: 2004. pp. 49–61.
-
- O’Neill J. 2015 Tackling a global health crisis: Initial steps. The Review on Antimicrobial Resistance Chaired by Jim O’Neill. Available at https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahU.... Accessed May 16, 2018.
-
- Davies SC. Annual Report of the Chief Medical Officer. Vol 2 Department of Health; London: 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
