

Effect of early physician follow-up on mortality and subsequent hospital admissions after emergency care for heart failure: a retrospective cohort study
- PMID: 30559279
- PMCID: PMC6291388
- DOI: 10.1503/cmaj.180786
Effect of early physician follow-up on mortality and subsequent hospital admissions after emergency care for heart failure: a retrospective cohort study
Abstract
Background: The 1-year mortality rate in patients with heart failure who are discharged from an emergency department is 20%. We sought to determine whether early follow-up after discharge from the emergency department was associated with decreased mortality or subsequent admission to hospital.
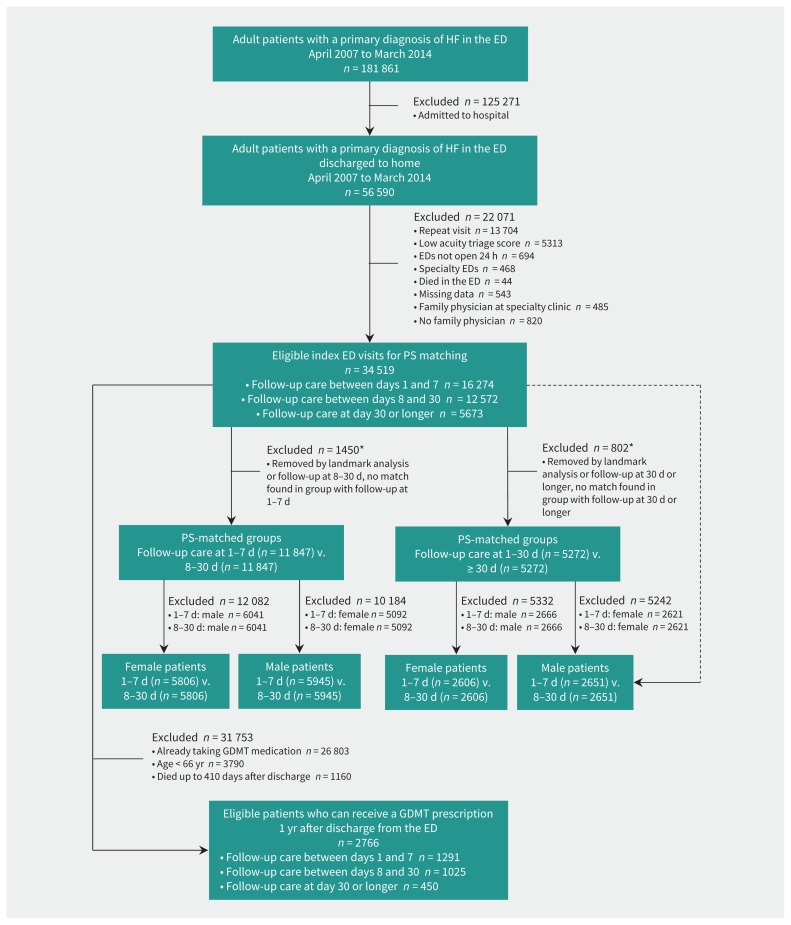
Methods: This retrospective cohort study conducted in Ontario, Canada, included adult patients who were discharged from 1 of 163 emergency departments between April 2007 and March 2014 with a primary diagnosis of heart failure. Using a propensity score-matched landmark analysis, we assessed follow-up in relation to mortality and admissions to hospital for cardiovascular conditions.
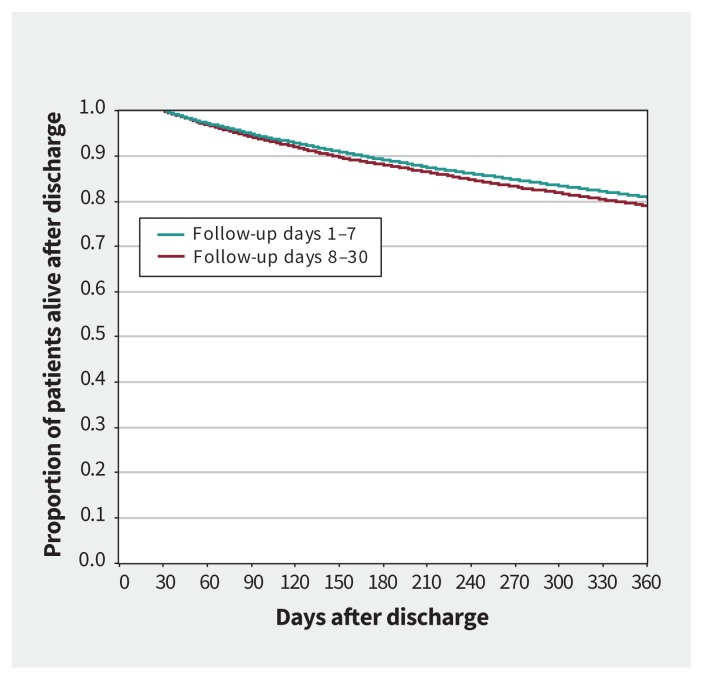
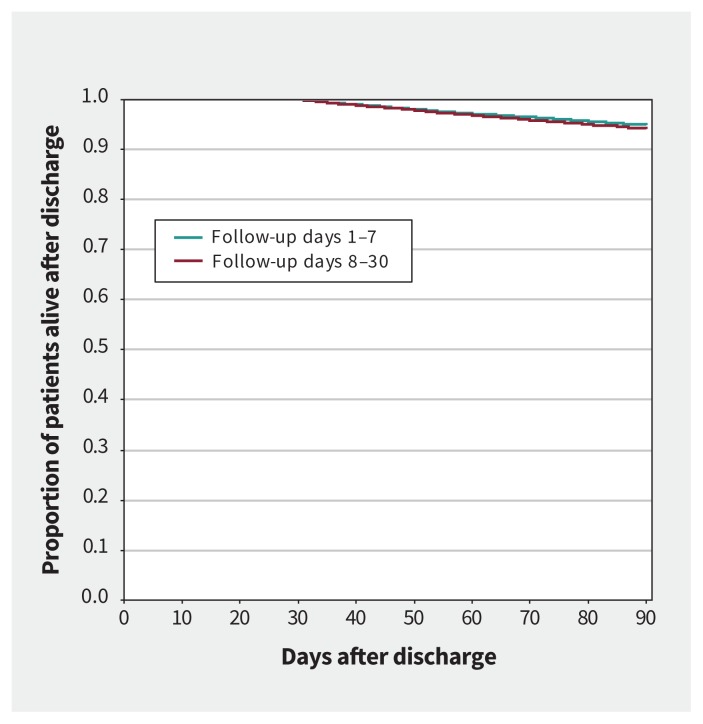
Results: Of 34 519 patients, 16 274 (47.1%) obtained follow-up care within 7 days and 28 846 (83.6%) within 30 days. Compared with follow-up between day 8 and 30, patients with follow-up care within 7 days had a lower rate of mortality over 1 year (hazard ratio [HR] 0.92; 95% confidence interval [CI] 0.87-0.97), and a reduced rate of admission to hospital over 90 days (HR 0.87, 95% CI 0.80-0.94) and 1 year (HR 0.92; 95% CI 0.87-0.97); the mortality rate over 90 days in this group trended to a lower rate (HR 0.90, 95% CI 0.10-1.00). Follow-up care within 30 days, compared with patients without 30-day follow-up, was associated with a reduction in 1-year mortality (HR 0.89, 95% CI 0.82-0.97) but not admission to hospital (HR 1.02, 95% CI 0.94-1.10). In this group, there was a trend toward an increase in 90-day admission to hospital (HR 1.14, 95% CI 1.00-1.29).
Interpretation: Follow-up care within 7 days of discharge from the emergency department was associated with lower rates of long-term mortality, as well as subsequent hospital admissions, and a trend to lower short-term mortality rates. Timely access to longitudinal care for patients with heart failure who are discharged from the emergency setting should be prioritized.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Effects of early physician follow-up.CMAJ. 2019 May 6;191(18):E509. doi: 10.1503/cmaj.71651. CMAJ. 2019. PMID: 31061079 Free PMC article. No abstract available.
References
-
- Singer AJ, Emerman C, Char DM, et al. Bronchodilator therapy in acute decompensated heart failure patients without a history of chronic obstructive pulmonary disease. Ann Emerg Med 2008;51:25–34. - PubMed
-
- Writing committee members Yancy CW, Jessup M, Bozkurt B, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013; 128:e240–327. - PubMed
-
- Hugli O, Braun JE, Kim S, et al. United States emergency department visits for acute decompensated heart failure, 1992 to 2001. Am J Cardiol 2005;96:1537–42. - PubMed
-
- Lee DS, Schull MJ, Alter DA, et al. Early deaths in patients with heart failure discharged from the emergency department: a population-based analysis. Circ Heart Fail 2010;3:228–35. - PubMed
-
- Ezekowitz JA, Bakal JA, Kaul P, et al. Acute heart failure in the emergency department: short and long-term outcomes of elderly patients with heart failure. Eur J Heart Fail 2008;10:308–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous