

Sarcomas of the breast: findings on mammography, ultrasound, and magnetic resonance imaging
- PMID: 30559558
- PMCID: PMC6290740
- DOI: 10.1590/0100-3984.2016.0141
Sarcomas of the breast: findings on mammography, ultrasound, and magnetic resonance imaging
Abstract
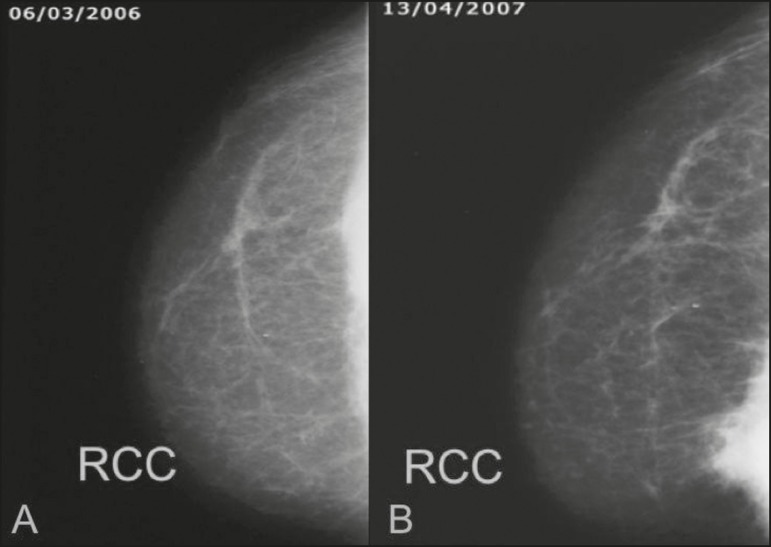
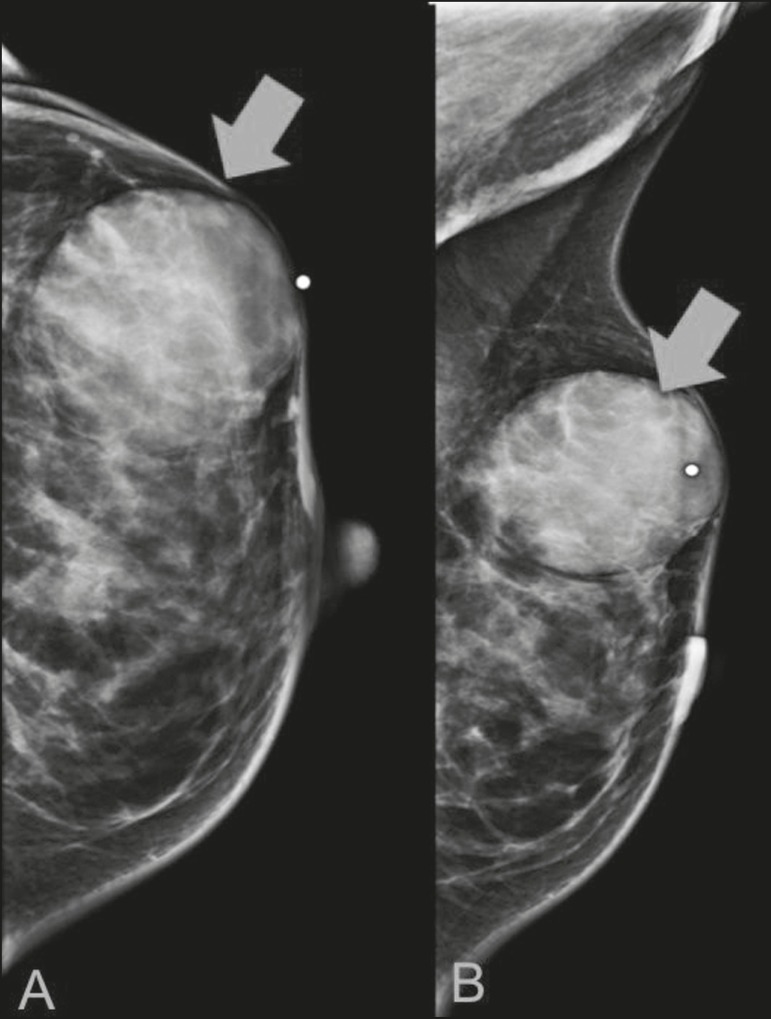
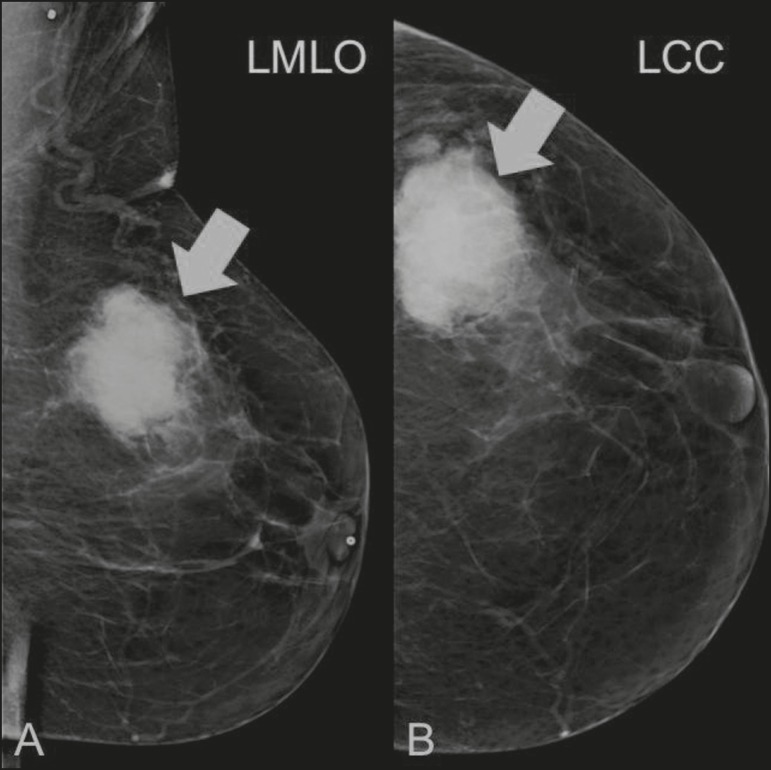
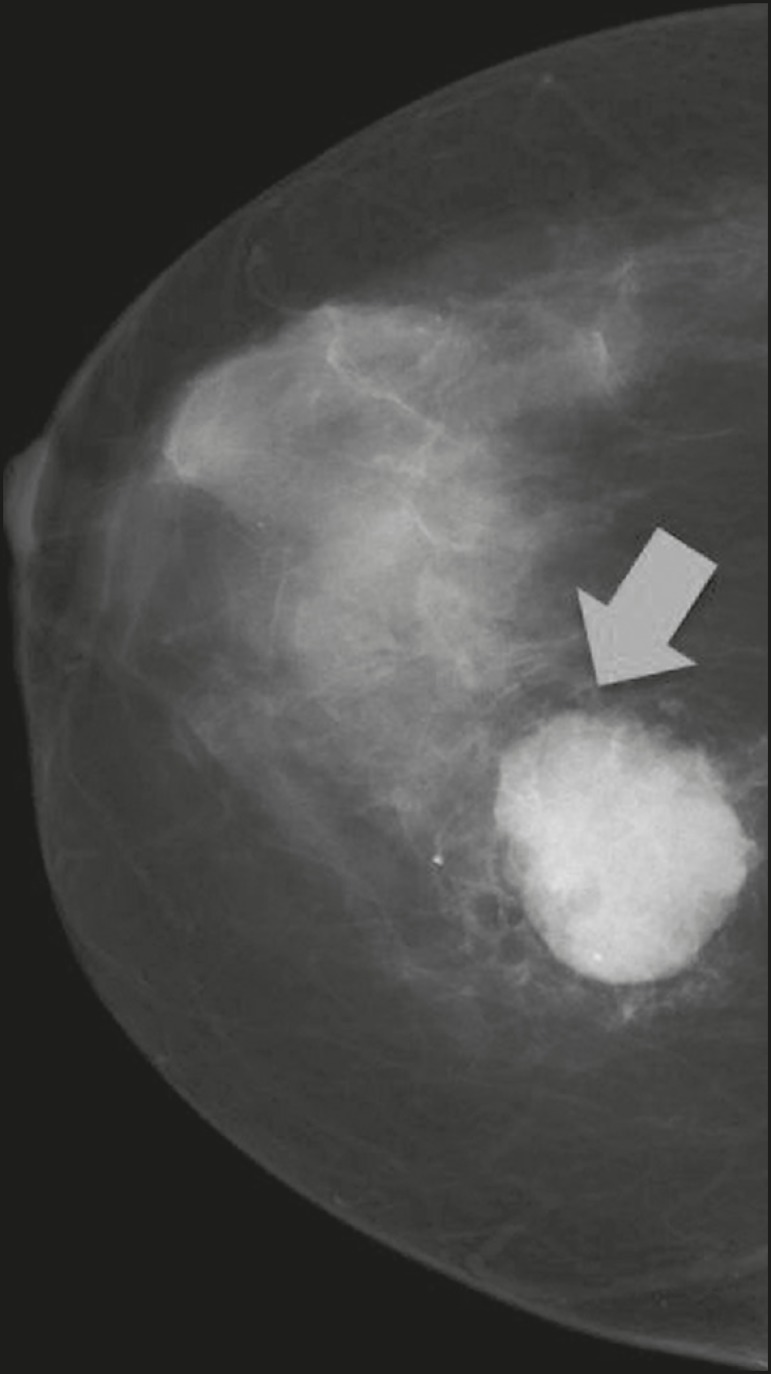
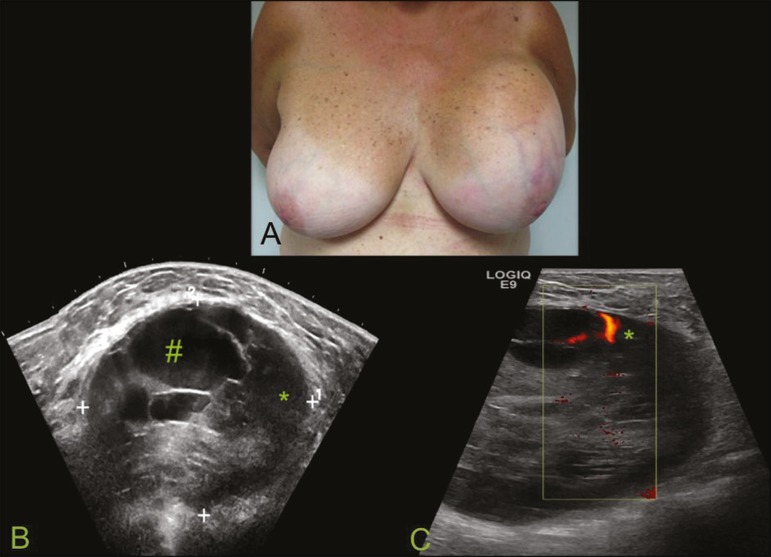
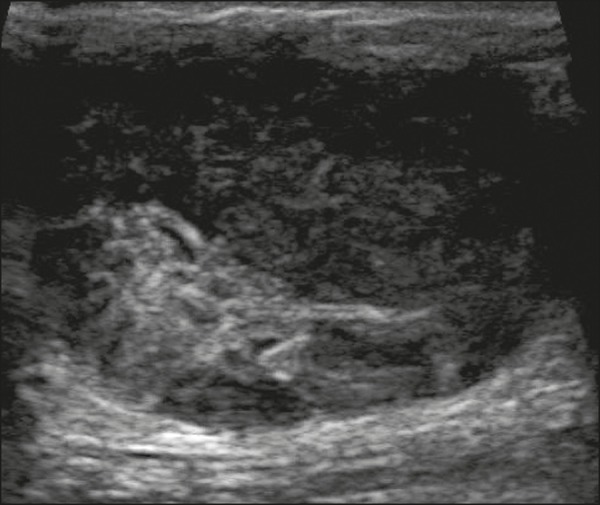
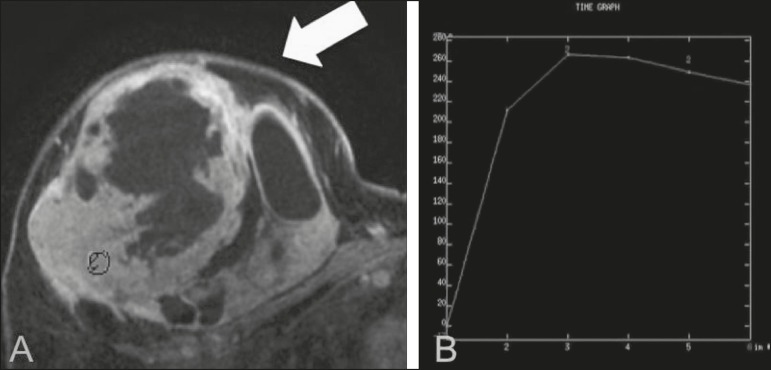
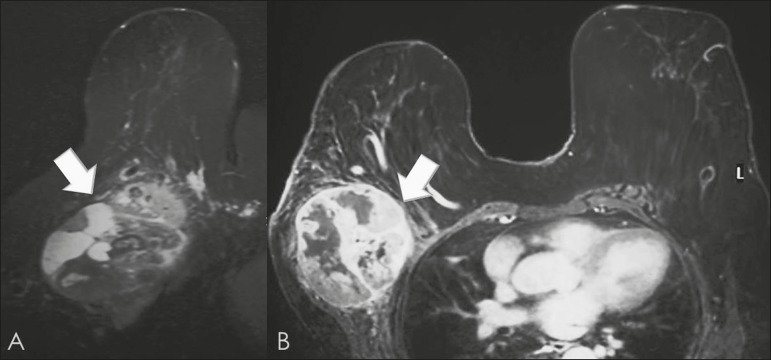
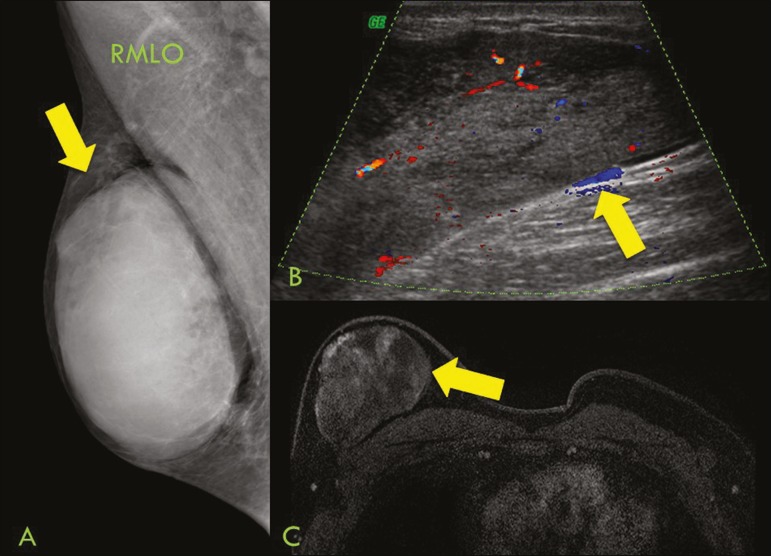
Sarcomas of the breast belong to a heterogeneous group of breast tumors of mesenchymal origin, without epithelial components. These tumors can be primary or secondary (after previous treatment for breast cancer), are rare, present aggressive behavior, and have a poor prognosis. They occur mainly in women between 45 and 50 years of age, with the exception of angiosarcomas, which can occur in younger patients. Clinically, breast sarcomas manifest as palpable, mobile, rapidly growing masses, without skin thickening, axillary lymphadenopathy, or nipple discharge. Although the imaging findings are non specific, they can be suggestive of sarcoma. For instance, a solitary mass showing rapid growth, with circumscribed or indistinct margins and, a complex (solid-cystic) or heterogeneous echotexture, without axillary lymph node involvement, can raise the suspicion of sarcoma. The treatment is not well established, because of the rarity and heterogeneity of this type of neoplasm. The principles of treatment for sarcoma of the breast have been addressed only in small cohort studies. In most cases, the treatment of choice is surgery without axillary lymphadenectomy.
Keywords: Breast cancer; Magnetic resonance imaging; Mammography; Sarcoma; Ultrasonography.
Figures

Similar articles
-
Imaging features of primary breast sarcoma: A case report.J Pak Med Assoc. 2021 Aug;71(8):2087-2089. doi: 10.47391/JPMA.05-706. J Pak Med Assoc. 2021. PMID: 34418037
-
Rare imaging appearance of adenoid cystic carcinoma of the breast: A case report.Mol Clin Oncol. 2017 Sep;7(3):473-475. doi: 10.3892/mco.2017.1322. Epub 2017 Jul 13. Mol Clin Oncol. 2017. PMID: 28781820 Free PMC article.
-
Inflammatory breast carcinoma: mammographic, ultrasonographic, clinical, and pathologic findings in 142 cases.Radiology. 2002 Jun;223(3):829-38. doi: 10.1148/radiol.2233010198. Radiology. 2002. PMID: 12034956
-
Breast metastases from extramammary malignancies: multimodality imaging aspects.Br J Radiol. 2017 Aug;90(1077):20170197. doi: 10.1259/bjr.20170197. Epub 2017 May 25. Br J Radiol. 2017. PMID: 28485985 Free PMC article. Review.
-
[A Breast Stromal Sarcoma-Case Report and Literature Review].Gan To Kagaku Ryoho. 2020 Jul;47(7):1093-1095. Gan To Kagaku Ryoho. 2020. PMID: 32668859 Review. Japanese.
Cited by
-
A rare case report of breast sarcoma.Radiol Case Rep. 2021 Feb 24;16(5):1047-1050. doi: 10.1016/j.radcr.2021.02.035. eCollection 2021 May. Radiol Case Rep. 2021. PMID: 33680274 Free PMC article.
-
Angiosarcoma of the Breast: Overview of Current Data and Multimodal Imaging Findings.J Imaging. 2023 Apr 30;9(5):94. doi: 10.3390/jimaging9050094. J Imaging. 2023. PMID: 37233313 Free PMC article. Review.
-
A 53-year-old female with a large breast sarcoma: A case report from Hong Kong.Radiol Case Rep. 2022 Jun 21;17(9):3055-3058. doi: 10.1016/j.radcr.2022.05.051. eCollection 2022 Sep. Radiol Case Rep. 2022. PMID: 35769124 Free PMC article.
-
Initial Imaging Findings of Breast Liposarcoma: A Case Report.Diagnostics (Basel). 2023 Jul 20;13(14):2428. doi: 10.3390/diagnostics13142428. Diagnostics (Basel). 2023. PMID: 37510172 Free PMC article.
-
Peripheral Neural Sheath Breast Sarcoma: Case Report and Literature Review.Case Rep Oncol. 2022 Apr 21;15(1):403-412. doi: 10.1159/000523811. eCollection 2022 Jan-Apr. Case Rep Oncol. 2022. PMID: 35702560 Free PMC article.
References
-
- McGowan TS, Cummings BJ, O'Sullivan B, et al. An analysis of 78 breast sarcoma patients without distant metastases at presentation. Int J Radiat Oncol Biol Phys. 2000;46:383–390. - PubMed
-
- Bousquet G, Confavreux C, Magné N, et al. Outcome and prognostic factors in breast sarcoma: a multicenter study from the rare cancer network. Radiother Oncol. 2007;85:355–361. - PubMed
-
- Al-Benna S, Poggemann K, Steinau HU, et al. Diagnosis and management of primary breast sarcoma. Breast Cancer Res Treat. 2010;122:619–626. - PubMed
-
- Lim SZ, Ong KW, Tan BKT, et al. Sarcoma of the breast: an update on a rare entity. J Clin Pathol. 2016;69:373–381. - PubMed
LinkOut - more resources
Full Text Sources