

Severe Acute Kidney Injury With Significant Uremia in an Infant Found to Have Inferior Vena Cava, Bilateral Renal Vein, and Bilateral Renal Artery Thromboses
- PMID: 30559631
- PMCID: PMC6292467
- DOI: 10.31486/toj.18.0051
Severe Acute Kidney Injury With Significant Uremia in an Infant Found to Have Inferior Vena Cava, Bilateral Renal Vein, and Bilateral Renal Artery Thromboses
Abstract
Background: Common neonatal etiologies of acute kidney injury (AKI) include renal vein and inferior vena cava thromboses, maternal use of nonsteroidal antiinflammatory drugs, and congenital renal disease. The incidence of renal vein thrombosis is estimated to be 0.5 per 1,000 neonatal intensive care unit admissions, with approximately half of cases extending to the inferior vena cava and with unilateral disease being significantly more common than bilateral. Data on abdominal venous thromboembolism in pediatric patients are limited, and the clinical presentation of renal vein thrombosis can vary, although most patients have at least one of the three cardinal signs: hematuria, thrombocytopenia, or abdominal mass.
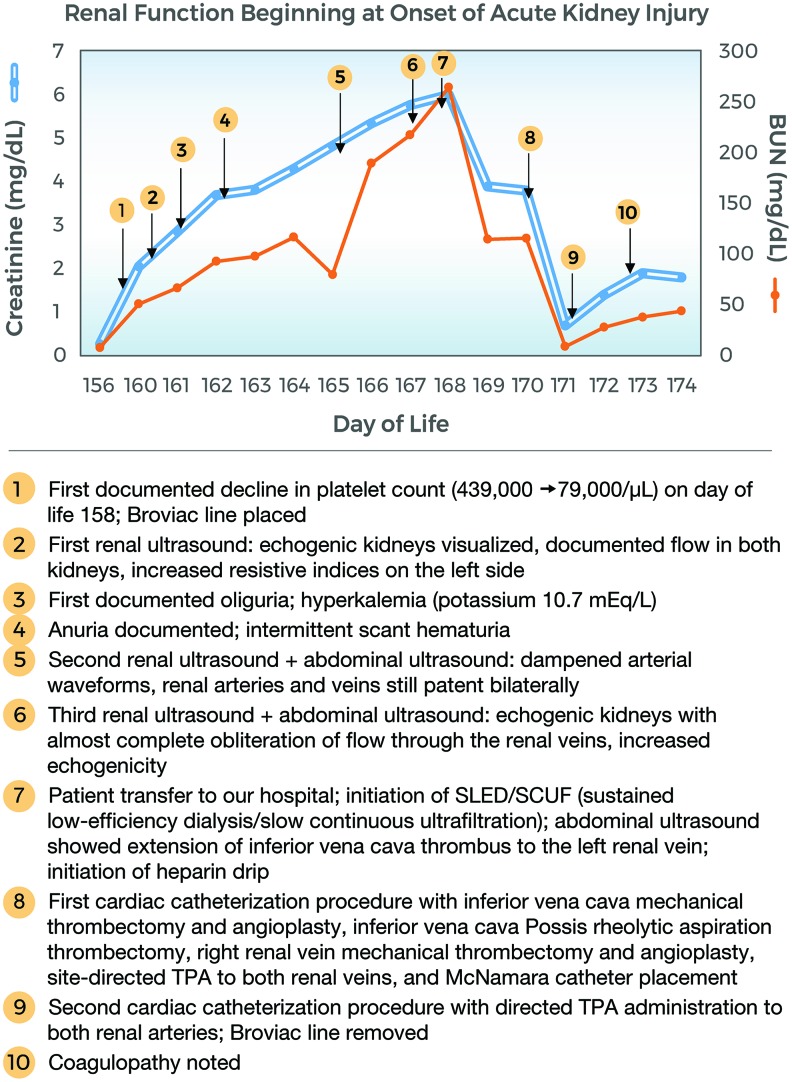
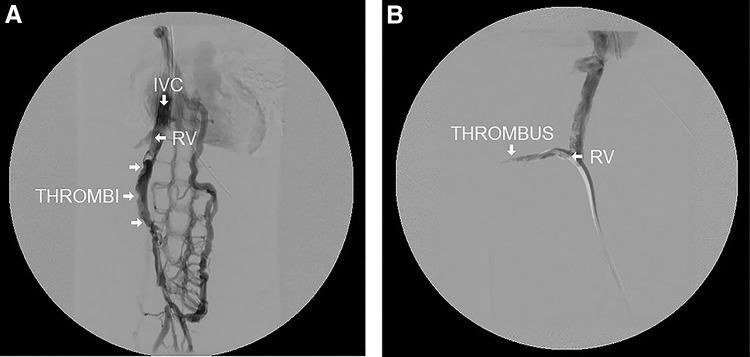
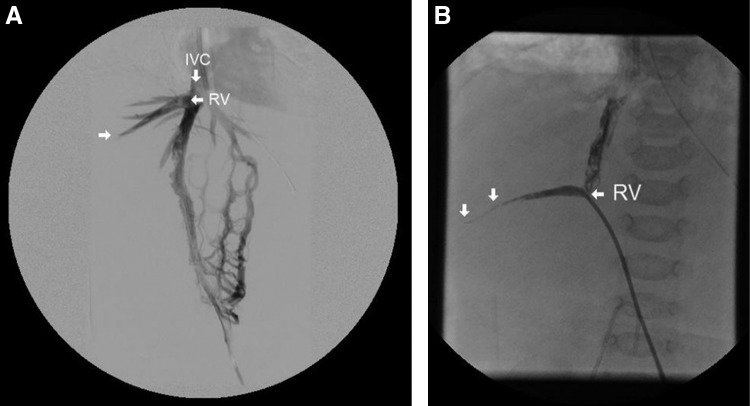
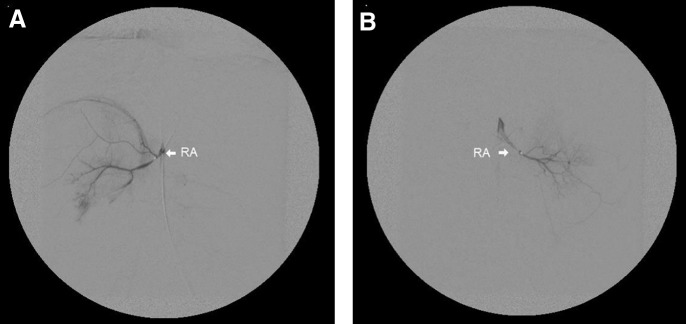
Case report: We present the case of a 5-month-old female transferred to our pediatric intensive care unit from an outside hospital with AKI and significant uremia (creatinine 6.01 mg/dL, blood urea nitrogen >200 mg/dL) secondary to inferior vena cava, bilateral renal vein, and bilateral renal artery thromboses. The patient was started on a heparin drip and subsequently underwent mechanical thrombectomy of her inferior vena cava and right renal vein in addition to site-directed tissue plasminogen activator to her renal veins, renal arteries, and inferior vena cava. Following the procedure, she developed severe coagulopathy and became hemodynamically labile. The coagulopathy was corrected, but further anticoagulation to prevent further thrombus propagation was not sustainable in the face of ongoing bleeding and hemodynamic instability, so the decision to withdraw mechanical support was made.
Conclusion: Because of the varied presentations of renal vein thrombosis and because prompt intervention significantly improves survival and renal outcomes, a high index of suspicion is warranted when risk factors and any of the three cardinal features of renal vein thrombosis are present.
Keywords: Acute kidney injury; anuria; intensive care–neonatal; intensive care–pediatric; thrombosis–venous; uremia.
Figures



References
-
- Section 2: AKI definition. Kidney Int Suppl (2011). 2012. March;2(1):19-36. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4089595/. Accessed September17, 2018. - PMC - PubMed
-
- Jetton JG, Rhone ET, Harer MW, Charlton JR, Selewski DT. Diagnosis and treatment of acute kidney injury in pediatrics. Curr Treat Options Pediatr. 2016. June;2(2):56-68. doi: 10.1007/s40746-016-0047-7. - DOI
-
- Flynn JT. Causes, management approaches, and outcome of acute renal failure in children. Curr Opin Pediatr. 1998. April;10(2):184-189. - PubMed
-
- Chan JC, Williams DM, Roth KS. Kidney failure in infants and children. Pediatr Rev. 2002. February;23(2):47-60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources