

A morphometric study of the structures bordering the infra-cochlear corridor - Relevant for endoscopic/microscopic ear surgery
- PMID: 30559770
- PMCID: PMC6291685
- DOI: 10.1016/j.joto.2018.08.001
A morphometric study of the structures bordering the infra-cochlear corridor - Relevant for endoscopic/microscopic ear surgery
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.J Otol. 2020 Dec;15(4):180. doi: 10.1016/j.joto.2020.10.001. Epub 2020 Oct 13. J Otol. 2020. PMID: 33293924 Free PMC article.
Abstract
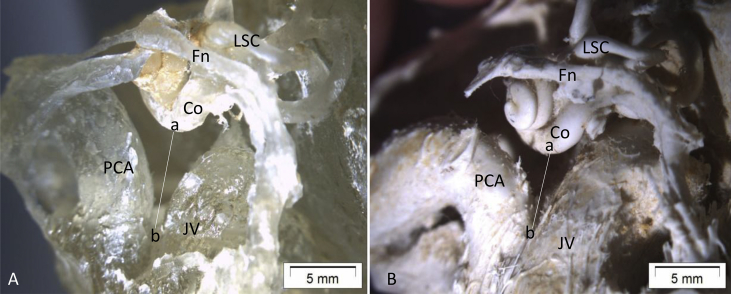
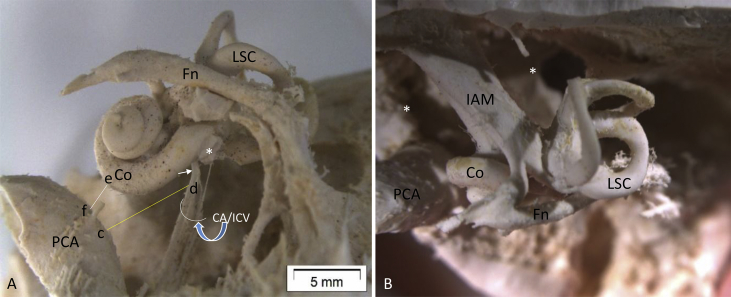
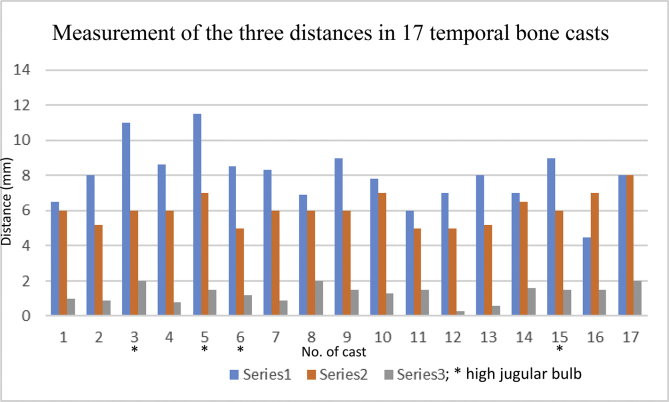
Application of surgical endoscope, used alone or in combination with the surgical microscope, for the operative management of ear and temporal bone conditions may allow improved access and clearance of disease. Preservation of normal structures may also be improved. As the use of this tool is increasing, the need for better understanding of the anatomy of the ear is becoming evident. This is particularly so for endoscopic surgery aiming at removal of lesions involving the infra-cochlear corridor and/or petrous apex. Human temporal bone-derived labyrinth casts (molds), originally made for endolymphatic duct and sac analysis which genuinely represent the membranous labyrinth and its adjacent soft tissues, were morphometrically analyzed in terms of the anatomic relations between structures in and around the infra-cochlear corridor. The distance between the petrous carotid artery (PCA) and the basal turn of the cochlea, the distance between PCA and infra-cochlear vein (ICV)/cochlear aqueduct (CA), and the distance between the lower surface of basal cochlear turn and the point where the carotid artery and jugular vein (JV) meet close to the jugular foramen, were measured to be around 1.3 mm, 6 mm and 8 mm respectively, thus constituting an approximate 6 × 8 mm2 infra-cochlear corridor. This analysis and further study with larger samples might be helpful for operation via this corridor led to the petrous apex where cholesterol granuloma, cholesteatoma and other lesions are not uncommon.
Keywords: Anatomical study; Ear endoscopy; Infra-cochlear corridor; Petrous apex; Surgery.
Figures
References
-
- Anson B.J., Donaldson J.A., Warpeha R.L., Winch T.R. The vestibular and cochlear aqueducts: their variational anatomy in the adult human ear. Laryngoscope. 1965;75:1203–1223. - PubMed
-
- Atturo F., Schart-Morén N., Larsson S., Rask-Andersen H., Li H. The human cochlear aqueduct and accessory canals: a micro-CT analysis using a 3D reconstruction paradigm. Otol. Neurotol. 2018;39(6):e429–e435. - PubMed
-
- Giddings N.A., Brackmann D.E., Kwartler J.A. Transcanal infracochlear approach to the petrous apex. Otolaryngology-Head Neck Surg. (Tokyo) 1991;104(1):29–36. - PubMed
-
- Guo R., Zhang H.L., Chen W., Zhu X.Q., Liu W., Helge Rask-Andersen H. The inferior cochlear vein: surgical aspects in cochlear implantation. Eur. Arch. Oto-Rhino-Laryngol. 2016;273:355–361. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
