

Does treatment of short or stunted children aged 6-59 months for severe acute malnutrition using ready to use therapeutic food make them overweight? Data from Malawi
- PMID: 30559964
- PMCID: PMC6292002
- DOI: 10.1186/s13690-018-0321-1
Does treatment of short or stunted children aged 6-59 months for severe acute malnutrition using ready to use therapeutic food make them overweight? Data from Malawi
Abstract
Background: Using mid-upper arm circumference (MUAC) to identify severe acute malnutrition (SAM) tends to identify younger and stunted children compared to alternative anthropometric case-definitions. It has been asserted by some experts, without supporting evidence, that stunted children with low MUAC may have normal weight for height and treatment with ready to use therapeutic food (RUTF) will cause excess adiposity, placing the child at risk for non-communicable diseases (NCD) later in life. It is recommended that children aged less than 6 months should not be treated with RUTF. Height cut-offs are frequently used in SAM treatment programmes to identify children likely to be aged less than 6 months and thus not eligible for treatment with RUTF. This is likely to exclude some stunted children aged 6 months or older. This study examined whether stunted children aged 6 months or older with SAM, identified by MUAC, and treated with RUTF were overweight or had excess adiposity when discharged cured with a MUAC of greater than 125 mm.
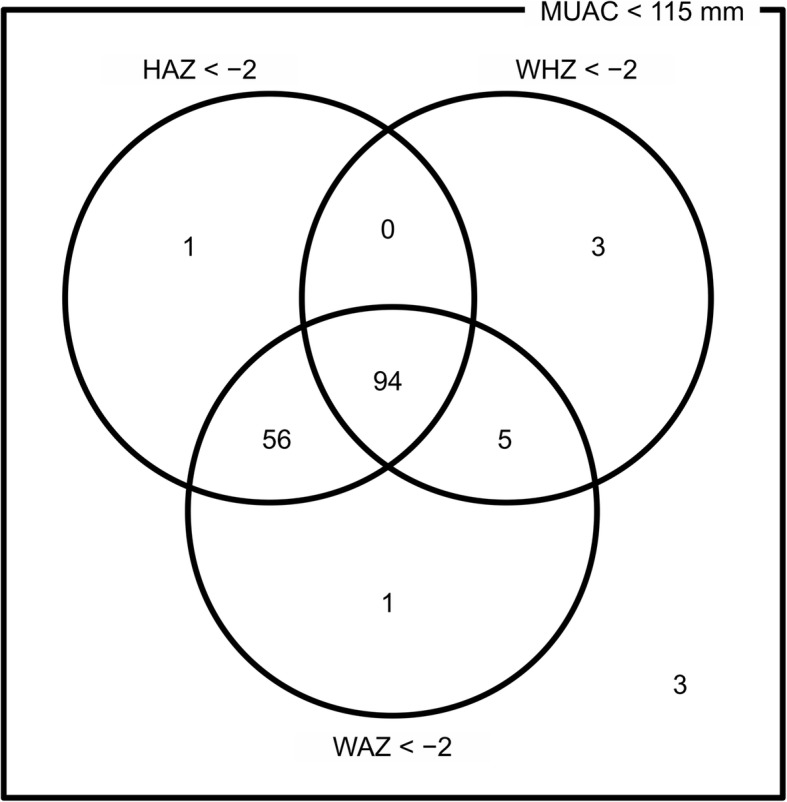
Methods: Data was collected at Ministry of Health primary health care facilities delivering community based management of acute malnutrition (CMAM) services between February 2011 and March 2012 in Lilongwe District, Malawi on 258 children aged between 6 and 59 months enrolled in outpatient treatment for SAM with a MUAC less than 115 mm without medical complications irrespective of height on admission. 163 children were discharged as cured when MUAC was 125 mm or greater and there was an absence of oedema and the child was clinically well for 2 consecutive visits. MUAC, triceps skin fold (TSF) thickness and weight were measured at each visit. Height was measured on admission and discharge.
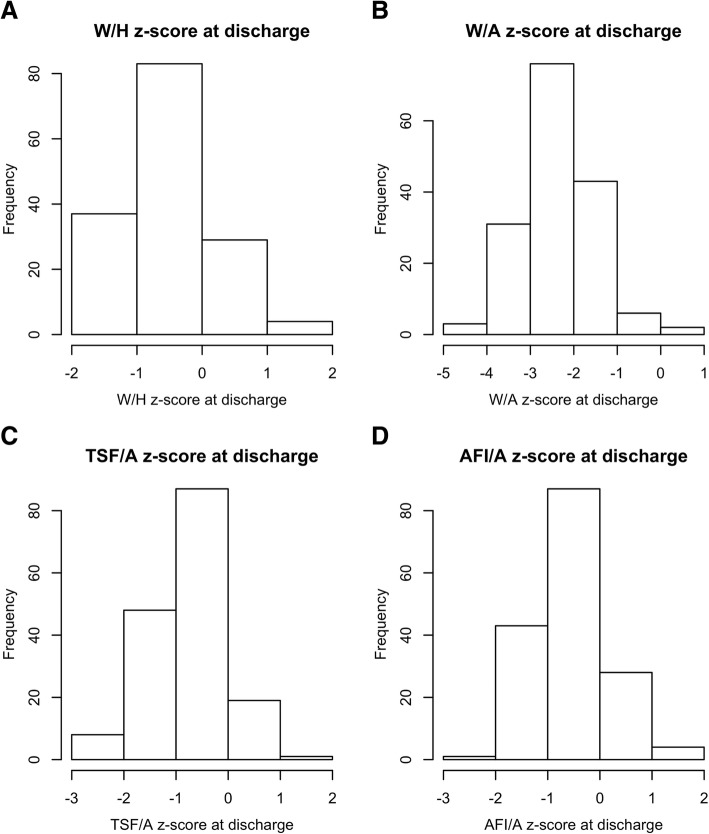
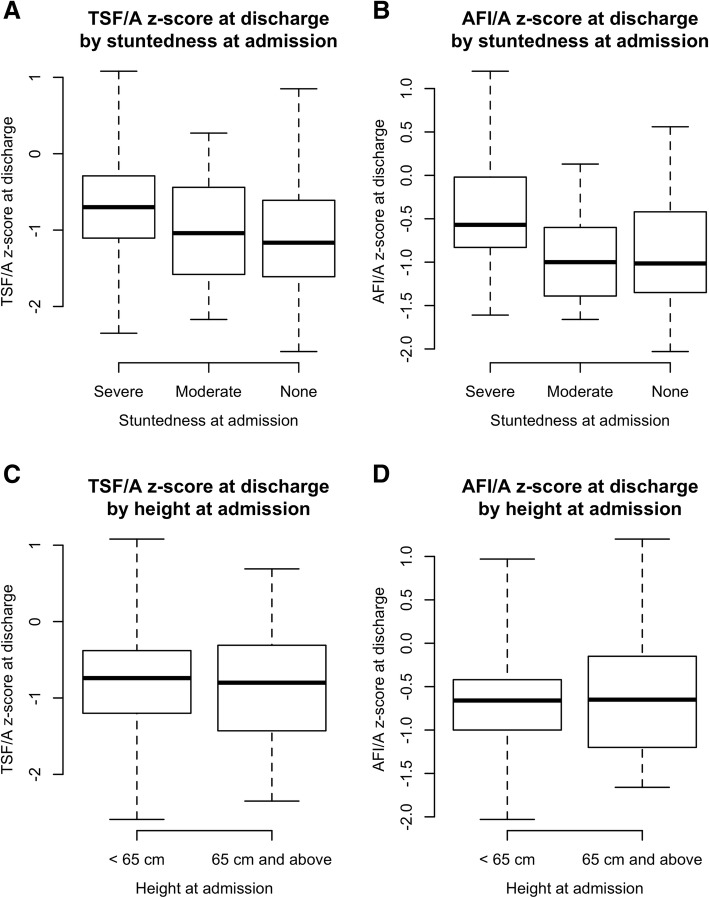
Results: No study subjects (n = 0) were overweight or had excess adiposity when discharged cured with a MUAC greater than 125 mm.. There was a tendency towards a higher TSF-for-age (TSF/A) z-scores for severely stunted children compared to non-stunted children (Kruskal-Wallis chi-squared = 9.0675, p-value = 0.0107). For children admitted with a height less than 65 cm and those with a height of 65 cm or greater, there was no significant difference in TSF/A z-scores on discharge (Kruskal-Wallis chi-squared = 0.9219, p = 0.3370) or AFI/A z-scores on discharge (Kruskal-Wallis chi-squared = 0.0740, p = 0.7855).
Conclusions: These results should allay concerns that children aged 6 months and older and with a height less than 65 cm or with severe stunting will become overweight or obese as a result of treatment with RUTF in the outpatient setting using recommended MUAC admission and discharge criteria.
Trial registration: ISRCTN 92405176 Registered 15th May 2018. Retrospectively registered.
Keywords: CMAM; MUAC; Overweight; RUTF; SAM; Stunting; Triceps skinfold thickness.
Conflict of interest statement
National Health Sciences Research Committee of Malawi, 30/11/2010, Protocol #817 MED/4/36. Written consent was obtained from a parent (or primary caregiver) of the child to be enrolled in the study. Each parent / caregiver signed an individual consent form detailing the proposed treatment, the right to refuse enrolment into the study, the right to confidentiality and anonymity, and that no payment would be received for participation. This study complied with World Medical Association Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects, 1964) and was approved by the National Health Sciences Research Committee of Malawi (NHSRC, protocol # 817).Not Applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO, WFP, UNSCN, UNICEF . Community-based Management of Severe Acute Malnutrition: a joint statement by the World Health Organization, the world food Programme, the United Nations system standing committee on nutrition and the United Nations Children’s fund. Geneva: World Health Organization, World Food Programme, United Nations System Standing Committee on Nutrition, United Nations Children’s Fund; 2007.
-
- Roberfroid et al. (2013) Utilisation of mid-upper arm circumference versus weight for height in nutritional rehabilitation programmes: a systematic review of evidence. Background Review 1 for the Updates on the management of severe acute malnutrition in infants and children. World Health Organisation, Geneva, 201. ISBN 978–92–4-150632-9 http://www.who.int/nutrition/publications/guidelines/updates_management_...
-
- Fabiansen, et al. Short children with a low mid-upper arm circumference respond to food supplementation: an observational study from Burkina Faso. Am J Clin Nutr doi. 2016. 10.3945/ajcn.115.124644. - PubMed
-
- Phelan, et al. Should we have height cut offs to define treatment for children with acute malnutrition? CMAM forum, FAQ. 2016.
-
- World Health Organisation . Guideline: updates on the management of severe acute malnutrition in infants and children. Geneva: World Health Organization; 2013. - PubMed
LinkOut - more resources
Full Text Sources
