

Uptake and radiological findings of screening cerebral magnetic resonance scans in patients with hereditary haemorrhagic telangiectasia
- PMID: 30560015
- PMCID: PMC6290842
- DOI: 10.5582/irdr.2018.01103
Uptake and radiological findings of screening cerebral magnetic resonance scans in patients with hereditary haemorrhagic telangiectasia
Abstract
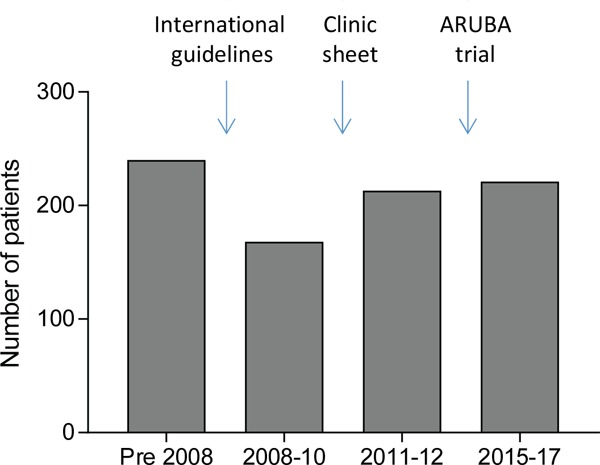
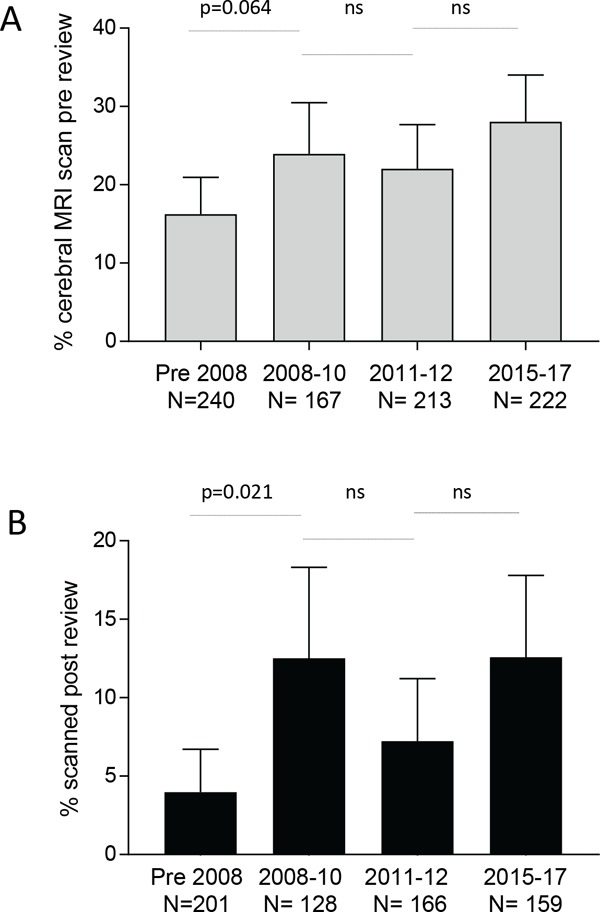
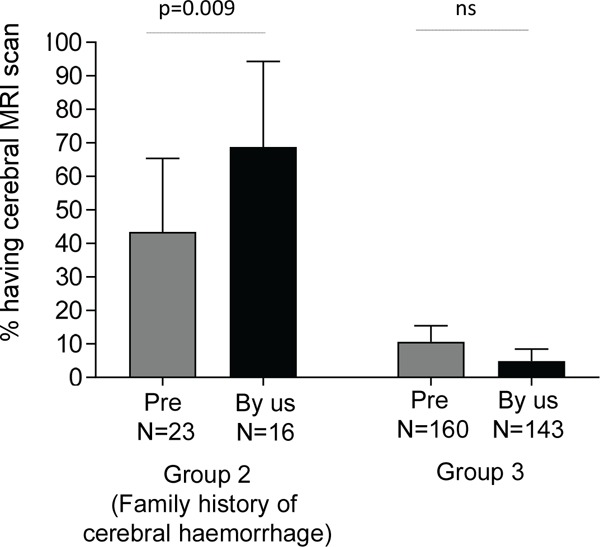
Hereditary haemorrhagic telangiectasia (HHT) results in arteriovenous malformations (AVMs), most commonly in the lungs, liver and brain. Discussion of cerebral vascular malformations is an important element of patient management. The current study objectives were to examine uptake and results of screening cerebral magnetic resonance (MR) scans, excluding symptomatic patients requiring neurological investigations. The remaining non-symptomatic individuals received formal pretest counselling that differed according to family history. For the 603 patients with no neurological symptoms of concern, screening scan uptake was higher after publication of the ARUBA trial. Patients with a family history of cerebral haemorrhage were 4 to 14-fold more likely to have a screening scan than patients with no such family history. For patients without neurological symptoms suggesting cerebral AVMs, none of the 59 screening scans performed at our institution demonstrated a cerebral AVM. Four scans (6.8%) demonstrated small aneurysms. The most common abnormality was cerebral infarction (20/59, 33.9%), predominantly identified in patients with pulmonary AVMs. Of 29 pulmonary AVM patients with no previous history of clinical stroke, 16 (55.2%) had between one and five silent infarcts. For HHT patients with pulmonary AVMs, the most frequently affected sites were the cerebellum (40%) and thalamus (14.3%), and the age-adjusted odds ratio for an infarct was 21.6 (95% confidence intervals 3.7, 126), p = 0.001. We concluded that for cerebral screening programmes in HHT, the findings support informed patient choice incorporating understanding that cerebral AVMs are rare in non-symptomatic HHT patients, but that screening scans commonly detect silent cerebral infarction due to pulmonary AVMs.
Keywords: Cerebral infarction; arteriovenous fistulas; cardioembolic stroke; counselling; magnetic resonance imaging; paradoxical emboli; pulmonary arteriovenous malformations; stroke.
Figures
References
-
- Shovlin CL. Hereditary haemorrhagic telangiectasia: Pathophysiology, diagnosis and treatment. Blood Rev. 2010; 24:203-219. - PubMed
-
- Kjeldsen AD, Vase P, Green A. Hereditary haemorrhagic telangiectasia: A population-based study of prevalence and mortality in Danish patients. J Intern Med. 1999; 245:31-39. - PubMed
-
- Bideau A, Brunet G, Heyer E, Plauchu H, Robert JM. An abnormal concentration of cases of Rendu-Osler disease in the Valserine valley of the French Jura: A geneological and demographic study. Ann of Hum Biol. 1992; 19:233-247. - PubMed
-
- Dakeishi M, Shioya T, Wada Y, Shindo T, Otaka K, Manabe M, Nozaki J, Inoue S, Koizumi A. Genetic epidemiology of hereditary hemorrhagic telangiectasia in a local community in the northern part of Japan. Hum Mutat. 2002; 19:140-148. - PubMed
-
- Westermann CJ, Rosina AF, De Vries V, de Coteau PA. The prevalence and manifestations of hereditary hemorrhagic telangiectasia in the Afro-Caribbean population of the Netherlands Antilles: A family screening. Am J Med Genet A. 2003; 116A:324-328. - PubMed
LinkOut - more resources
Full Text Sources
Medical