

Effects of Antibiotic Cycling Policy on Incidence of Healthcare-Associated MRSA and Clostridioides difficile Infection in Secondary Healthcare Settings
- PMID: 30561306
- PMCID: PMC6302607
- DOI: 10.3201/eid2501.180111
Effects of Antibiotic Cycling Policy on Incidence of Healthcare-Associated MRSA and Clostridioides difficile Infection in Secondary Healthcare Settings
Abstract
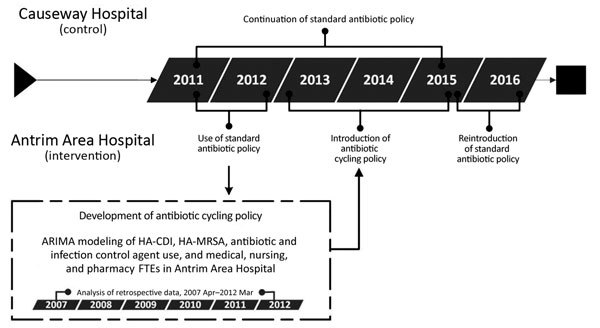
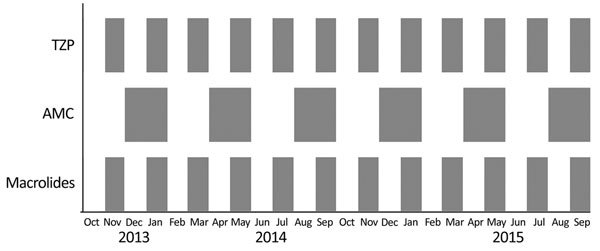
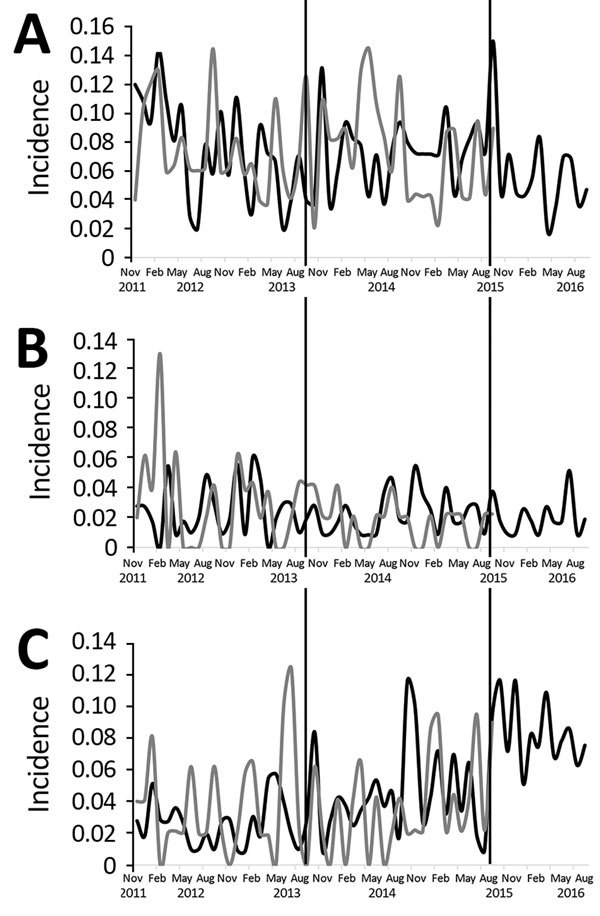
This quasi-experimental study investigated the effect of an antibiotic cycling policy based on time-series analysis of epidemiologic data, which identified antimicrobial drugs and time periods for restriction. Cyclical restrictions of amoxicillin/clavulanic acid, piperacillin/tazobactam, and clarithromycin were undertaken over a 2-year period in the intervention hospital. We used segmented regression analysis to compare the effect on the incidence of healthcare-associated Clostridioides difficile infection (HA-CDI), healthcare-associated methicillin-resistant Staphylococcus aureus (HA-MRSA), and new extended-spectrum β-lactamase (ESBL) isolates and on changes in resistance patterns of the HA-MRSA and ESBL organisms between the intervention and control hospitals. HA-CDI incidence did not change. HA-MRSA incidence increased significantly in the intervention hospital. The resistance of new ESBL isolates to amoxicillin/clavulanic acid and piperacillin/tazobactam decreased significantly in the intervention hospital; however, resistance to piperacillin/tazobactam increased after a return to the standard policy. The results question the value of antibiotic cycling to antibiotic stewardship.
Keywords: CDI; Clostridioides difficile; Clostridium difficile; ESBL; Ireland; MRSA; antibiotic cycling; antimicrobial drug resistance; bacteria; extended-spectrum β-lactamase; healthcare-acquired infections; methicillin-resistant Staphylococcus aureus; nosocomial infections.
Figures

References
-
- Ashiru-Oredope D, Budd EL, Bhattacharya A, Din N, McNulty CA, Micallef C, et al. ; English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR). Implementation of antimicrobial stewardship interventions recommended by national toolkits in primary and secondary healthcare sectors in England: TARGET and Start Smart Then Focus. J Antimicrob Chemother. 2016;71:1408–14. 10.1093/jac/dkv492 - DOI - PubMed
-
- Ashiru-Oredope D, Hopkins S; English Surveillance Programme for Antimicrobial Utilization and Resistance Oversight Group. Antimicrobial stewardship: English Surveillance Programme for Antimicrobial Utilization and Resistance (ESPAUR). J Antimicrob Chemother. 2013;68:2421–3. 10.1093/jac/dkt363 - DOI - PubMed
-
- Aldeyab MA, Scott MG, Kearney MP, Alahmadi YM, Magee FA, Conlon G, et al. Impact of an enhanced antibiotic stewardship on reducing methicillin-resistant Staphylococcus aureus in primary and secondary healthcare settings. Epidemiol Infect. 2014;142:494–500. 10.1017/S0950268813001374 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
