

Association of Delivery Mode With Pelvic Floor Disorders After Childbirth
- PMID: 30561480
- PMCID: PMC6583632
- DOI: 10.1001/jama.2018.18315
Association of Delivery Mode With Pelvic Floor Disorders After Childbirth
Abstract
Importance: Pelvic floor disorders (eg, urinary incontinence), which affect approximately 25% of women in the United States, are associated with childbirth. However, little is known about the course and progression of pelvic floor disorders over time.
Objective: To describe the incidence of pelvic floor disorders after childbirth and identify maternal and obstetrical characteristics associated with patterns of incidence 1 to 2 decades after delivery.
Design, setting, and participants: Women were recruited from a community hospital for this cohort study 5 to 10 years after their first delivery and followed up annually for up to 9 years. Recruitment was based on mode of delivery; delivery groups were matched for age and years since first delivery. Of 4072 eligible women, 1528 enrolled between October 2008 and December 2013. Annual follow-up continued through April 2017.
Exposures: Participants were categorized into the following mode of delivery groups: cesarean birth (cesarean deliveries only), spontaneous vaginal birth (≥1 spontaneous vaginal delivery and no operative vaginal deliveries), or operative vaginal birth (≥1 operative vaginal delivery).
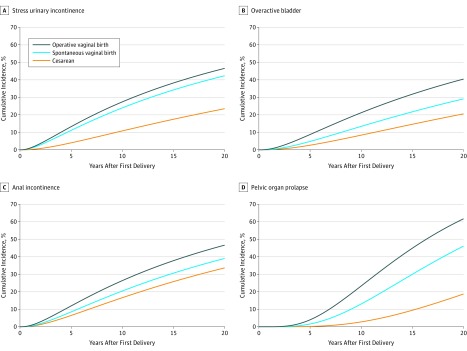
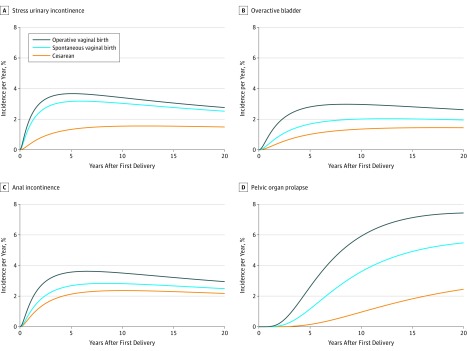
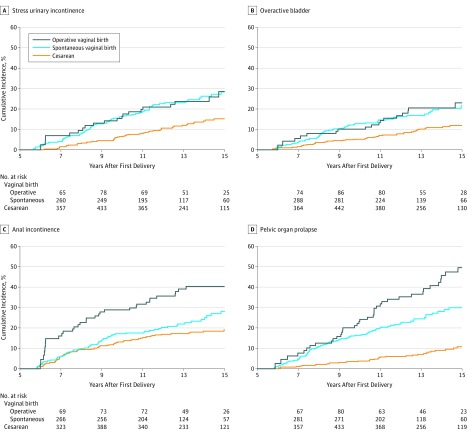
Main outcomes and measures: Stress urinary incontinence (SUI), overactive bladder (OAB), and anal incontinence (AI), defined using validated threshold scores from the Epidemiology of Prolapse and Incontinence Questionnaire, and pelvic organ prolapse (POP), measured using the Pelvic Organ Prolapse Quantification Examination. Cumulative incidences, by delivery group, were estimated using parametric methods. Hazard ratios, by exposure, were estimated using semiparametric models.
Results: Among 1528 women (778 in the cesarean birth group, 565 in the spontaneous vaginal birth group, and 185 in the operative vaginal birth group), the median age at first delivery was 30.6 years, 1092 women (72%) were multiparous at enrollment (2887 total deliveries), and the median age at enrollment was 38.3 years. During a median follow-up of 5.1 years (7804 person-visits), there were 138 cases of SUI, 117 cases of OAB, 168 cases of AI, and 153 cases of POP. For spontaneous vaginal delivery (reference), the 15-year cumulative incidences of pelvic floor disorders after first delivery were as follows: SUI, 34.3% (95% CI, 29.9%-38.6%); OAB, 21.8% (95% CI, 17.8%-25.7%); AI, 30.6% (95% CI, 26.4%-34.9%), and POP, 30.0% (95% CI, 25.1%-34.9%). Compared with spontaneous vaginal delivery, cesarean delivery was associated with significantly lower hazard of SUI (adjusted hazard ratio [aHR], 0.46 [95% CI, 0.32-0.67]), OAB (aHR, 0.51 [95% CI, 0.34-0.76]), and POP (aHR, 0.28 [95% CI, 0.19-0.42]), while operative vaginal delivery was associated with significantly higher hazard of AI (aHR, 1.75 [95% CI, 1.14-2.68]) and POP (aHR, 1.88 [95% CI, 1.28-2.78]). Stratifying by delivery mode, the hazard ratios for POP, relative to a genital hiatus size less than or equal to 2.5 cm, were 3.0 (95% CI, 1.7-5.3) for a genital hiatus size of 3 cm and 9.0 (95% CI, 5.5-14.8) for a genital hiatus size greater than or equal to 3.5 cm.
Conclusions and relevance: Compared with spontaneous vaginal delivery, cesarean delivery was associated with significantly lower hazard for stress urinary incontinence, overactive bladder, and pelvic organ prolapse, while operative vaginal delivery was associated with significantly higher hazard of anal incontinence and pelvic organ prolapse. A larger genital hiatus was associated with increased risk of pelvic organ prolapse independent of delivery mode.
Conflict of interest statement
Figures
Comment in
-
Re: Association of Delivery Mode with Pelvic Floor Disorders after Childbirth.J Urol. 2019 Oct;202(4):651. doi: 10.1097/JU.0000000000000442. Epub 2019 Sep 6. J Urol. 2019. PMID: 31294660 No abstract available.
-
Impact of Vaginal Delivery on Pelvic Floor.Rev Bras Ginecol Obstet. 2020 Feb;42(2):65-66. doi: 10.1055/s-0040-1709184. Epub 2020 Mar 30. Rev Bras Ginecol Obstet. 2020. PMID: 32227320 Free PMC article. No abstract available.
References
-
- Vincent GK, Velkoff VA. The Next Four Decades–the Older Population in the United States: 2010 to 2050. Washington, DC: US Census Bureau; 2010. https://www.census.gov/prod/2010pubs/p25-1138.pdf.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
