

Opioids for Chronic Noncancer Pain: A Systematic Review and Meta-analysis
- PMID: 30561481
- PMCID: PMC6583638
- DOI: 10.1001/jama.2018.18472
Opioids for Chronic Noncancer Pain: A Systematic Review and Meta-analysis
Abstract
Importance: Harms and benefits of opioids for chronic noncancer pain remain unclear.
Objective: To systematically review randomized clinical trials (RCTs) of opioids for chronic noncancer pain.
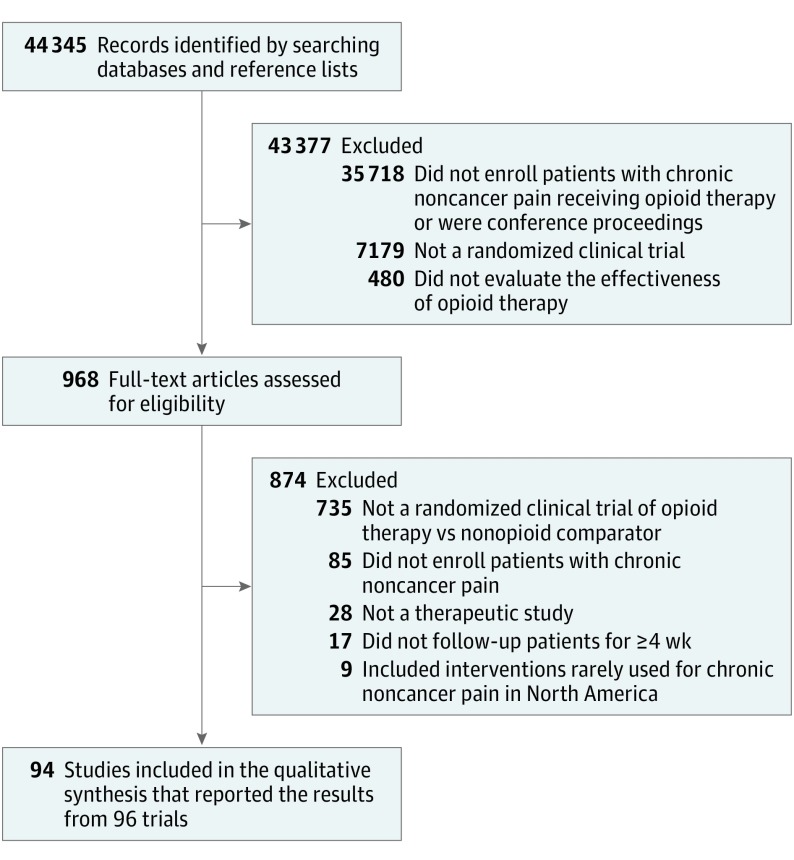
Data sources and study selection: The databases of CENTRAL, CINAHL, EMBASE, MEDLINE, AMED, and PsycINFO were searched from inception to April 2018 for RCTs of opioids for chronic noncancer pain vs any nonopioid control.
Data extraction and synthesis: Paired reviewers independently extracted data. The analyses used random-effects models and the Grading of Recommendations Assessment, Development and Evaluation to rate the quality of the evidence.
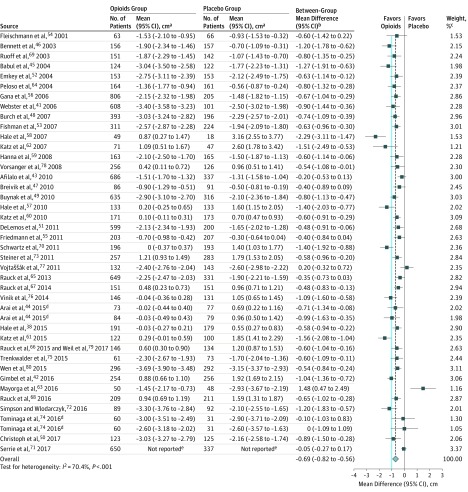
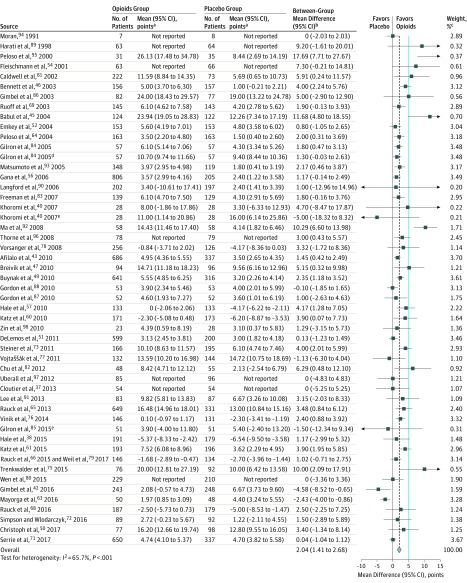
Main outcomes and measures: The primary outcomes were pain intensity (score range, 0-10 cm on a visual analog scale for pain; lower is better and the minimally important difference [MID] is 1 cm), physical functioning (score range, 0-100 points on the 36-item Short Form physical component score [SF-36 PCS]; higher is better and the MID is 5 points), and incidence of vomiting.
Results: Ninety-six RCTs including 26 169 participants (61% female; median age, 58 years [interquartile range, 51-61 years]) were included. Of the included studies, there were 25 trials of neuropathic pain, 32 trials of nociceptive pain, 33 trials of central sensitization (pain present in the absence of tissue damage), and 6 trials of mixed types of pain. Compared with placebo, opioid use was associated with reduced pain (weighted mean difference [WMD], -0.69 cm [95% CI, -0.82 to -0.56 cm] on a 10-cm visual analog scale for pain; modeled risk difference for achieving the MID, 11.9% [95% CI, 9.7% to 14.1%]), improved physical functioning (WMD, 2.04 points [95% CI, 1.41 to 2.68 points] on the 100-point SF-36 PCS; modeled risk difference for achieving the MID, 8.5% [95% CI, 5.9% to 11.2%]), and increased vomiting (5.9% with opioids vs 2.3% with placebo for trials that excluded patients with adverse events during a run-in period). Low- to moderate-quality evidence suggested similar associations of opioids with improvements in pain and physical functioning compared with nonsteroidal anti-inflammatory drugs (pain: WMD, -0.60 cm [95% CI, -1.54 to 0.34 cm]; physical functioning: WMD, -0.90 points [95% CI, -2.69 to 0.89 points]), tricyclic antidepressants (pain: WMD, -0.13 cm [95% CI, -0.99 to 0.74 cm]; physical functioning: WMD, -5.31 points [95% CI, -13.77 to 3.14 points]), and anticonvulsants (pain: WMD, -0.90 cm [95% CI, -1.65 to -0.14 cm]; physical functioning: WMD, 0.45 points [95% CI, -5.77 to 6.66 points]).
Conclusions and relevance: In this meta-analysis of RCTs of patients with chronic noncancer pain, evidence from high-quality studies showed that opioid use was associated with statistically significant but small improvements in pain and physical functioning, and increased risk of vomiting compared with placebo. Comparisons of opioids with nonopioid alternatives suggested that the benefit for pain and functioning may be similar, although the evidence was from studies of only low to moderate quality.
Conflict of interest statement
Figures
Comment in
-
Increasing Evidence for the Limited Role of Opioids to Treat Chronic Noncancer Pain.JAMA. 2018 Dec 18;320(23):2427-2428. doi: 10.1001/jama.2018.19327. JAMA. 2018. PMID: 30561463 No abstract available.
-
Review: Opioids improve chronic noncancer pain, but difference may not be clinically meaningful in most patients.Ann Intern Med. 2019 Apr 16;170(8):JC41. doi: 10.7326/ACPJ201904160-041. Ann Intern Med. 2019. PMID: 30986831 No abstract available.
-
Meta-analysis of Opioids for Chronic Pain.JAMA. 2019 May 21;321(19):1934-1935. doi: 10.1001/jama.2019.2177. JAMA. 2019. PMID: 31112253 No abstract available.
-
Meta-analysis of Opioids for Chronic Pain.JAMA. 2019 May 21;321(19):1935-1936. doi: 10.1001/jama.2019.2181. JAMA. 2019. PMID: 31112254 No abstract available.
References
-
- International Narcotics Control Board Narcotic drugs: estimated world requirements for 2017: statistics for 2015. https://www.incb.org/documents/Narcotic-Drugs/Technical-Publications/201.... Accessed October 25, 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
