

National Burden of Heart Failure Events in the United States, 2006 to 2014
- PMID: 30562099
- PMCID: PMC6424109
- DOI: 10.1161/CIRCHEARTFAILURE.117.004873
National Burden of Heart Failure Events in the United States, 2006 to 2014
Abstract
Background: Heart failure (HF)-a serious and costly condition-is increasingly prevalent. We estimated the US burden including emergency department (ED) visits, inpatient hospitalizations and associated costs, and mortality.
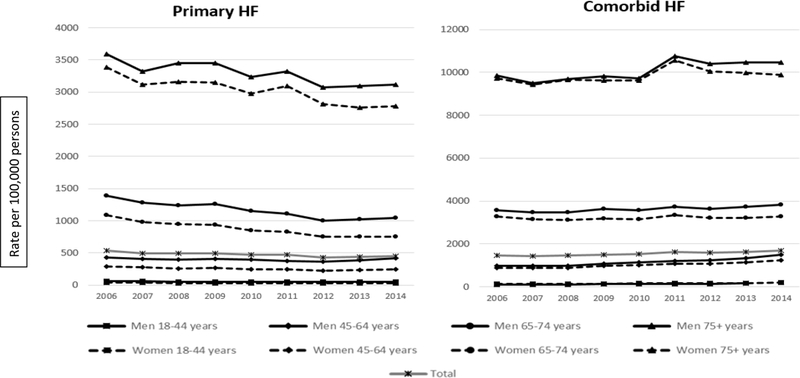
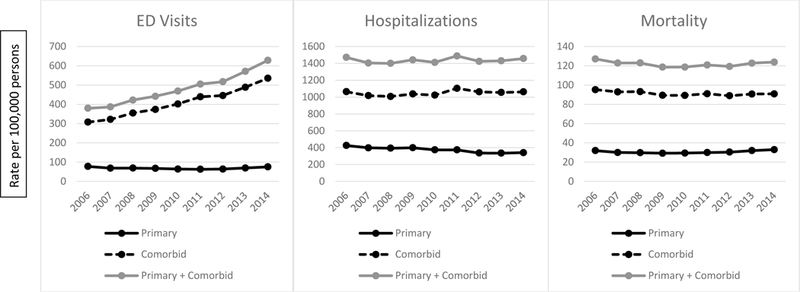
Methods and results: We analyzed 2006 to 2014 data from the Healthcare Cost and Utilization Project Nationwide Emergency Department Sample, the Healthcare Cost and Utilization Project National (nationwide) Inpatient Sample, and the National Vital Statistics System. International Classification of Disease codes identified HF and comorbidities. Burden was estimated separately for ED visits, hospitalizations, and mortality. In addition, criteria were applied to identify total unique acute events. Rates of primary HF (primary diagnosis or underlying cause of death) and comorbid HF (comorbid diagnosis or contributing cause of death) were calculated, age standardized to the 2010 US population. In 2014, there were an estimated 1 068 412 ED visits, 978 135 hospitalizations, and 83 705 deaths with primary HF. There were 4 071 546 ED visits, 3 370 856 hospitalizations, and 230 963 deaths with comorbid HF. Between 2006 and 2014, the total unique acute event rate for primary HF declined from 536 to 449 per 100 000 (relative percent change of -16%; P for trend, <0.001) but increased for comorbid HF from 1467 to 1689 per 100 000 (relative percentage change, 15%; P for trend, <0.001). HF-related mortality decreased significantly from 2006 to 2009 but did not change meaningfully after 2009. For hospitalizations with primary HF, the estimated mean cost was $11 552 in 2014, totaling an estimated $11 billion.
Conclusions: Given substantial healthcare and mortality burden of HF, rising healthcare costs, and the aging US population, continued improvements in HF prevention, management, and surveillance are important.
Keywords: United States; comorbidity; heart failure; hospitalization; humans.
Conflict of interest statement
Conflict of Interest Disclosures
None
Figures
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS and Muntner P. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. Circulation. 2017:e16–e458. - PMC - PubMed
-
- Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ and Levy D. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106:3068–3072. - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Pina IL and Trogdon JG. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circulation Heart failure. 2013;6:606–619. - PMC - PubMed
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KKL, Murabito JM and Vasan RS. Long-Term Trends in the Incidence of and Survival with Heart Failure. New England Journal of Medicine. 2002;347:1397–1402. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
