

Predictive Score for Identifying Survival and Recurrence Risk Profiles in Patients Undergoing Ventricular Tachycardia Ablation: The I-VT Score
- PMID: 30562104
- PMCID: PMC6301075
- DOI: 10.1161/CIRCEP.118.006730
Predictive Score for Identifying Survival and Recurrence Risk Profiles in Patients Undergoing Ventricular Tachycardia Ablation: The I-VT Score
Abstract
Background: Several distinct risk factors for arrhythmia recurrence and mortality following ventricular tachycardia (VT) ablation have been described. The effect of concurrent risk factors has not been assessed so far; thus, it is not yet possible to estimate these risks for a patient with several comorbidities. The aim of the study was to identify specific risk groups for mortality and VT recurrence using the Survival Tree (ST) analysis method.
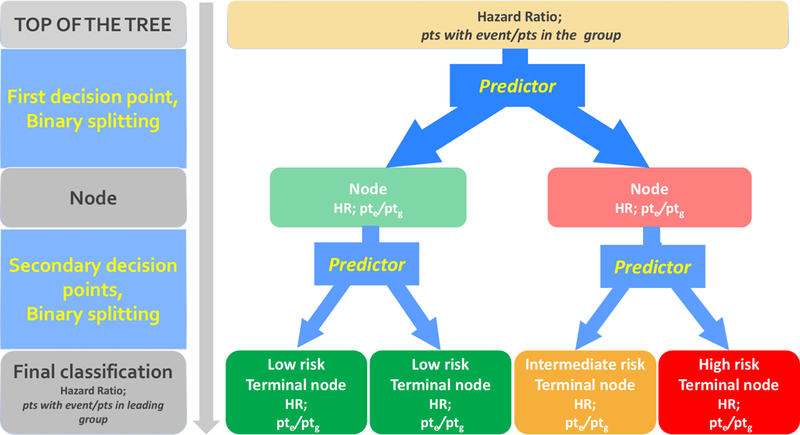
Methods: In 1251 patients 16 demographic, clinical and procedure-related variables were evaluated as potential prognostic factors using ST analysis using a recursive partitioning algorithm that searches for relationships among variables. Survival time and time to VT recurrence in groups derived from ST analysis were compared by a log-rank test. A random forest analysis was then run to extract a variable importance index and internally validate the ST models.
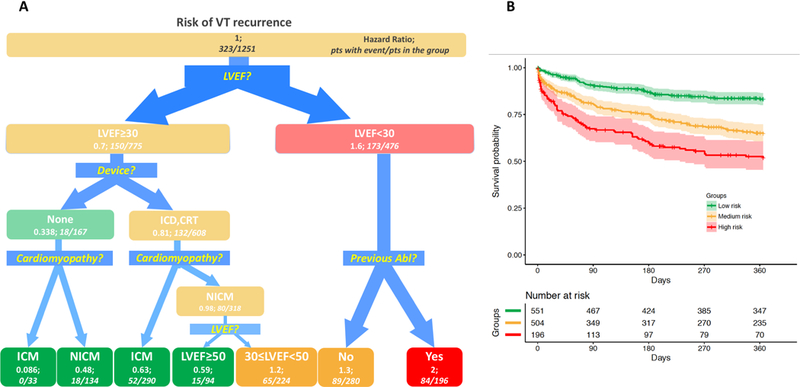
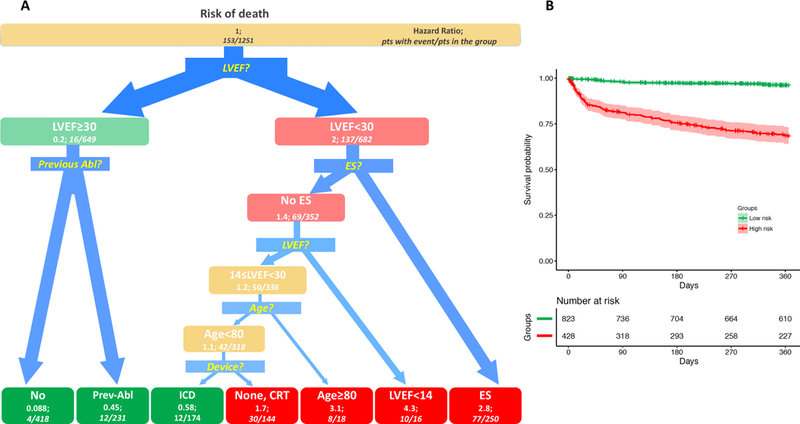
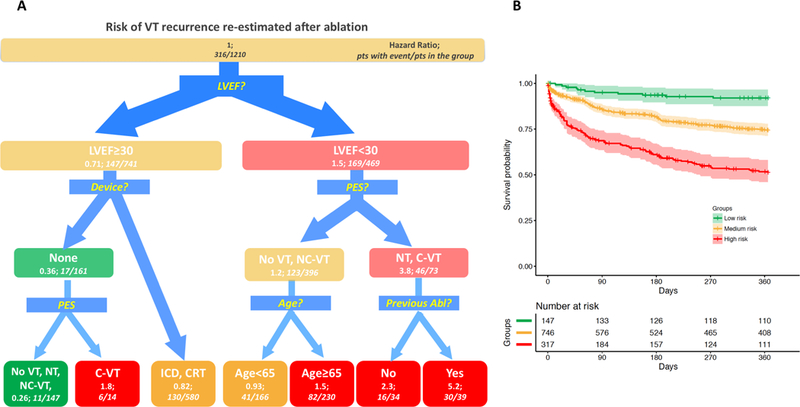
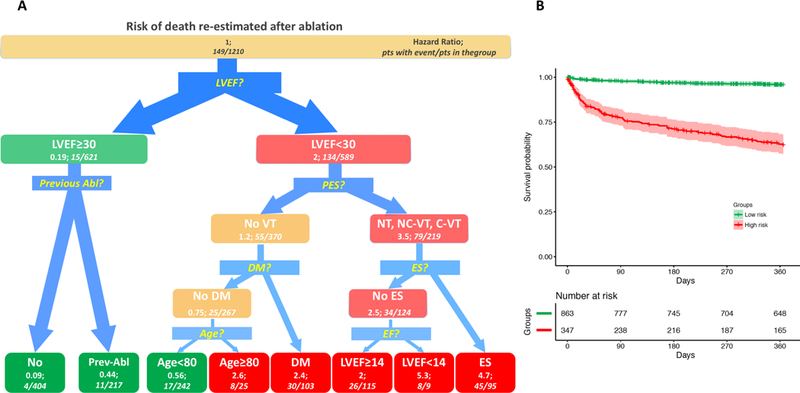
Results: Left ventricular ejection fraction, implantable cardioverter defibrillator/cardiac resynchronization device, previous ablation were, in hierarchical order, identified by ST analysis as best predictors of VT recurrence, while left ventricular ejection fraction, previous ablation, Electrical storm were identified as best predictors of mortality. Three groups with significantly different survival rates were identified. Among the high-risk group, 65.0% patients were survived and 52.1% patients were free from VT recurrence; within the medium- and low-risk groups, 84.0% and 97.2% patients survived, 72.4% and 88.4% were free from VT recurrence, respectively.
Conclusions: Our study is the first to derive and validate a decisional model that provides estimates of VT recurrence and mortality with an effective classification tree. Preprocedure risk stratification could help optimize periprocedural and postprocedural care.
Keywords: cardiomyopathies; catheter ablation; mortality; risk assessment; ventricular tachycardia.
Figures
Similar articles
-
Noninvasive programmed ventricular stimulation early after ventricular tachycardia ablation to predict risk of late recurrence.J Am Coll Cardiol. 2012 Apr 24;59(17):1529-35. doi: 10.1016/j.jacc.2012.01.026. J Am Coll Cardiol. 2012. PMID: 22516442
-
Long-term outcome of catheter ablation and other form of therapy for electrical storm in patients with implantable cardioverter-defibrillators.J Interv Card Electrophysiol. 2017 Dec;50(3):227-234. doi: 10.1007/s10840-017-0291-1. Epub 2017 Oct 24. J Interv Card Electrophysiol. 2017. PMID: 29064045 Free PMC article.
-
Noninducibility and late potential abolition: a novel combined prognostic procedural end point for catheter ablation of postinfarction ventricular tachycardia.Circ Arrhythm Electrophysiol. 2014 Jun;7(3):424-35. doi: 10.1161/CIRCEP.113.001239. Epub 2014 May 15. Circ Arrhythm Electrophysiol. 2014. PMID: 24833642
-
Ventricular Tachycardia with ICD Shocks: When to Medicate and When to Ablate.Curr Cardiol Rep. 2017 Sep 13;19(11):105. doi: 10.1007/s11886-017-0924-0. Curr Cardiol Rep. 2017. PMID: 28900864 Review.
-
Catheter Ablation of Ventricular Tachycardia in Patients With a Ventricular Assist Device: A Systematic Review of Procedural Characteristics and Outcomes.JACC Clin Electrophysiol. 2019 Jan;5(1):39-51. doi: 10.1016/j.jacep.2018.08.009. Epub 2018 Sep 26. JACC Clin Electrophysiol. 2019. PMID: 30678785
Cited by
-
Acute haemodynamic decompensation in the era of substrate-based ablation: rare but still worrisome.Europace. 2024 Jun 3;26(6):euae144. doi: 10.1093/europace/euae144. Europace. 2024. PMID: 38864731 Free PMC article. No abstract available.
-
Complications and mortality after catheter ablation of ventricular arrhythmias: risk in VT ablation (RIVA) score.Clin Res Cardiol. 2022 May;111(5):530-540. doi: 10.1007/s00392-021-01902-2. Epub 2021 Jul 27. Clin Res Cardiol. 2022. PMID: 34318341 Free PMC article.
-
Catheter Ablation for Ventricular Tachycardia in Patients With Biopsy-Proven Myocarditis.JACC Asia. 2024 Oct 22;4(12):1000-1009. doi: 10.1016/j.jacasi.2024.08.018. eCollection 2024 Dec. JACC Asia. 2024. PMID: 39802997 Free PMC article.
-
Lipomatous Metaplasia Is Associated With Ventricular Tachycardia Recurrence Following Ablation in Patients With Nonischemic Cardiomyopathy.JACC Clin Electrophysiol. 2024 Jun;10(6):1135-1146. doi: 10.1016/j.jacep.2024.02.024. Epub 2024 May 1. JACC Clin Electrophysiol. 2024. PMID: 38703163 Free PMC article.
-
Machine-Learning-Based Prediction of 1-Year Arrhythmia Recurrence after Ventricular Tachycardia Ablation in Patients with Structural Heart Disease.Bioengineering (Basel). 2023 Dec 1;10(12):1386. doi: 10.3390/bioengineering10121386. Bioengineering (Basel). 2023. PMID: 38135977 Free PMC article.
References
-
- Kuck KH, Schaumann A, Eckardt L, Willems S, Ventura R, Delacretaz E, Pitschner HF, Kautzner J, Schumacher B and Hansen PS. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet. 2010;375:31–40. - PubMed
-
- Sapp JL, Wells GA, Parkash R, Stevenson WG, Blier L, Sarrazin JF, Thibault B, Rivard L, Gula L, Leong-Sit P, Essebag V, Nery PB, Tung SK, Raymond JM, Sterns LD, Veenhuyzen GD, Healey JS, Redfearn D, Roux JF and Tang AS. Ventricular Tachycardia Ablation versus Escalation of Antiarrhythmic Drugs. N Engl J Med. 2016;375:111–21. - PubMed
-
- Palaniswamy C, Kolte D, Harikrishnan P, Khera S, Aronow WS, Mujib M, Mellana WM, Eugenio P, Lessner S, Ferrick A, Fonarow GC, Ahmed A, Cooper HA, Frishman WH, Panza JA and Iwai S. Catheter ablation of postinfarction ventricular tachycardia: ten-year trends in utilization, in-hospital complications, and in-hospital mortality in the United States. Heart Rhythm. 2014;11:2056–63. - PubMed
-
- Priori SG, Blomstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekval TM, Spaulding C and Van Veldhuisen DJ. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36:2793–867. - PubMed
