

Recent Advances in Oncolytic Virotherapy and Immunotherapy for Glioblastoma: A Glimmer of Hope in the Search for an Effective Therapy?
- PMID: 30563098
- PMCID: PMC6316815
- DOI: 10.3390/cancers10120492
Recent Advances in Oncolytic Virotherapy and Immunotherapy for Glioblastoma: A Glimmer of Hope in the Search for an Effective Therapy?
Abstract
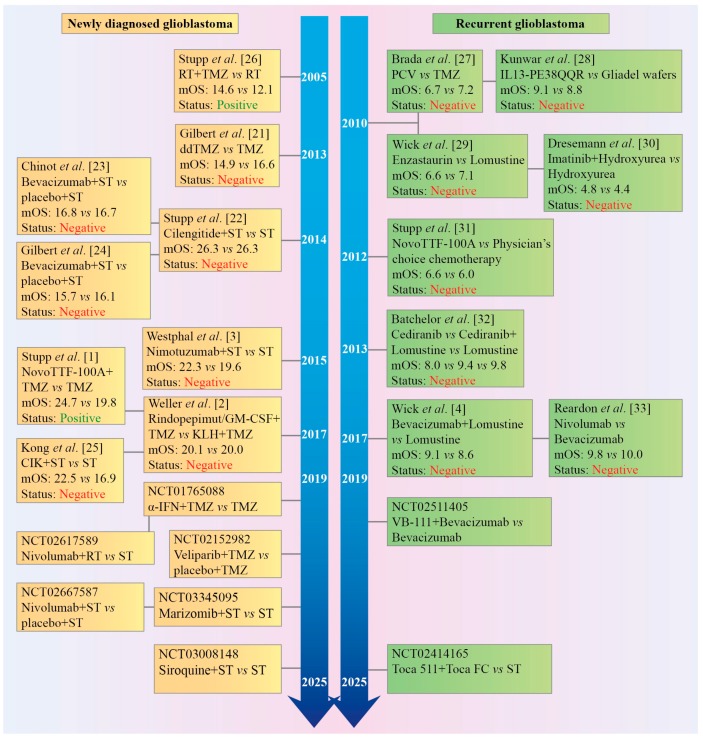
To date, no targeted drugs, antibodies or combinations of chemotherapeutics have been demonstrated to be more efficient than temozolomide, or to increase efficacy of standard therapy (surgery, radiotherapy, temozolomide, steroid dexamethasone). According to recent phase III trials, standard therapy may ensure a median overall survival of up to 18⁻20 months for adult patients with newly diagnosed glioblastoma. These data explain a failure of positive non-controlled phase II trials to predict positive phase III trials and should result in revision of the landmark Stupp trial as a historical control for median overall survival in non-controlled trials. A high rate of failures in clinical trials and a lack of effective chemotherapy on the horizon fostered the development of conceptually distinct therapeutic approaches: dendritic cell/peptide immunotherapy, chimeric antigen receptor (CAR) T-cell therapy and oncolytic virotherapy. Recent early phase trials with the recombinant adenovirus DNX-2401 (Ad5-delta24-RGD), polio-rhinovirus chimera (PVSRIPO), parvovirus H-1 (ParvOryx), Toca 511 retroviral vector with 5-fluorocytosine, heat shock protein-peptide complex-96 (HSPPC-96) and dendritic cell vaccines, including DCVax-L vaccine, demonstrated that subsets of patients with glioblastoma/glioma may benefit from oncolytic virotherapy/immunotherapy (>3 years of survival after treatment). However, large controlled trials are required to prove efficacy of next-generation immunotherapeutics and oncolytic vectors.
Keywords: PD-L1; TTFields; bevacizumab; dendritic cell vaccine; glioma; immunotherapy; oncolytic virotherapy; radiotherapy; targeted drugs; temozolomide.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Stupp R., Taillibert S., Kanner A., Read W., Steinberg D., Lhermitte B., Toms S., Idbaih A., Ahluwalia M.S., Fink K., et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA. 2017;318:2306–2316. doi: 10.1001/jama.2017.18718. - DOI - PMC - PubMed
-
- Weller M., Butowski N., Tran D.D., Recht L.D., Lim M., Hirte H., Ashby L., Mechtler L., Goldlust S.A., Iwamoto F., et al. Rindopepimut with temozolomide for patients with newly diagnosed, EGFRvIII-expressing glioblastoma (ACT IV): A randomised, double-blind, international phase 3 trial. Lancet Oncol. 2017;18:1373–1385. doi: 10.1016/S1470-2045(17)30517-X. - DOI - PubMed
-
- Westphal M., Heese O., Steinbach J.P., Schnell O., Schackert G., Mehdorn M., Schulz D., Simon M., Schlegel U., Senft C., et al. A randomised, open label phase III trial with nimotuzumab, an anti-epidermal growth factor receptor monoclonal antibody in the treatment of newly diagnosed adult glioblastoma. Eur. J. Cancer. 2015;51:522–532. doi: 10.1016/j.ejca.2014.12.019. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
