

Reduced Plasma Levels of Very-Long-Chain Dicarboxylic Acid 28:4 in Italian and Brazilian Colorectal Cancer Patient Cohorts
- PMID: 30563293
- PMCID: PMC6316647
- DOI: 10.3390/metabo8040091
Reduced Plasma Levels of Very-Long-Chain Dicarboxylic Acid 28:4 in Italian and Brazilian Colorectal Cancer Patient Cohorts
Abstract
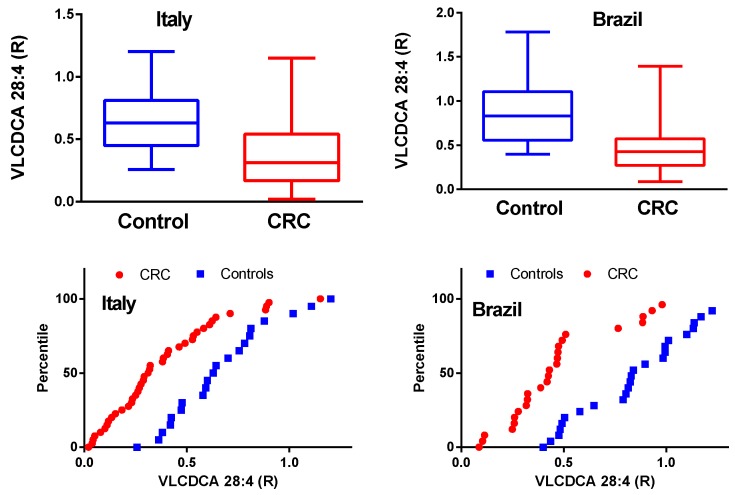
Background: There are currently no blood-based biomarkers for early diagnosis of colorectal cancer. Previous research has suggested that very-long-chain dicarboxylic acid (VLCDCA) 28:4 might be such a biomarker.
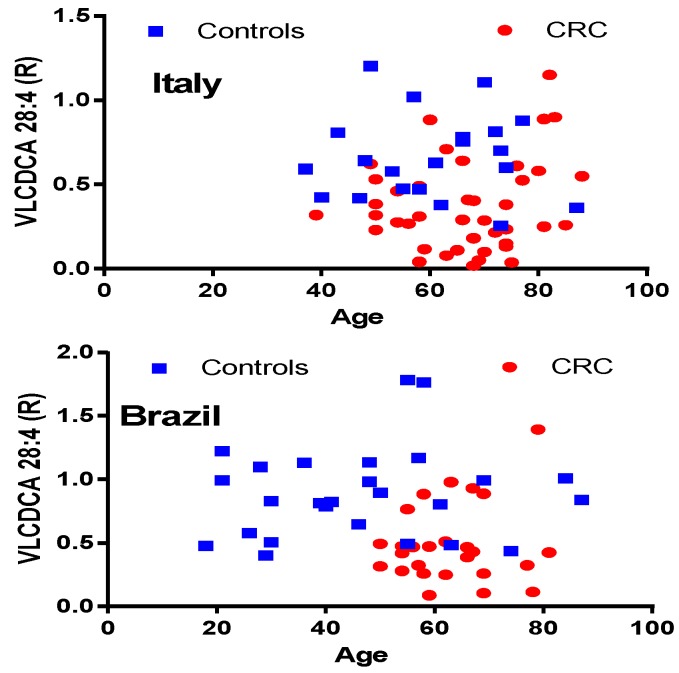
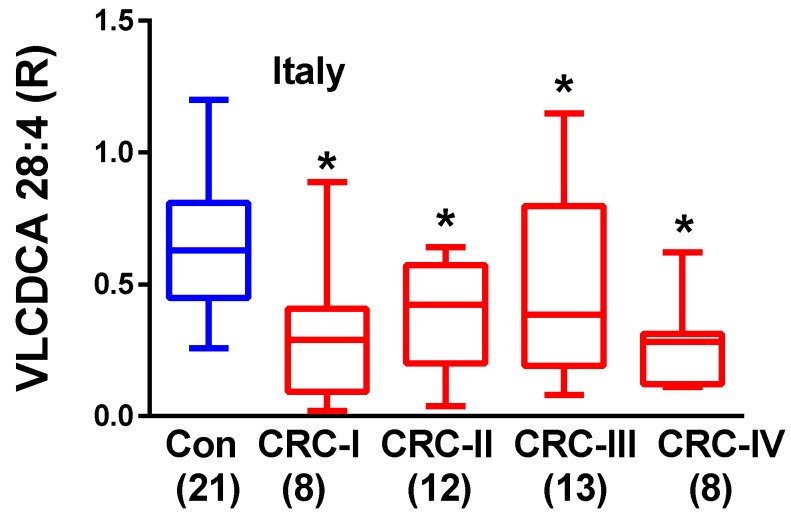
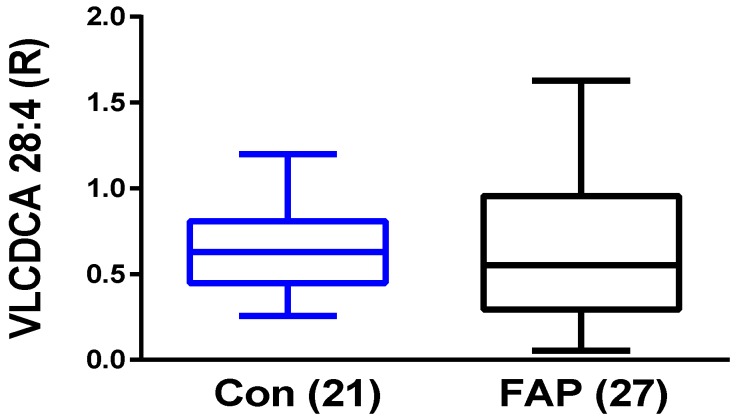
Methods: Using high-resolution mass spectrometry, we analyzed VLCDCA 28:4 in the plasma of colorectal cancer patients in Italian [n = 62] and Brazilian [n = 52] cohorts. Additionally, we investigated individuals diagnosed with familial adenomatous polyposis (FAP; n = 27), one of the most important clinical forms of inherited susceptibility to colorectal cancer. Results: Decrements in plasma levels of VLCDCA 28:4 were monitored in colorectal cancer patients. These decreases were independent of the stage of tumor development and the individual's age. However, no decrements in VLCDCA 28:4 were monitored in FAP patients.
Conclusions: The plasma levels of VLCDCA 28:4 represent a potential biomarker of sporadic colorectal cancer. In addition, it is possible that resupply of this anti-inflammatory lipid may represent a new therapeutic strategy for CRC and inflammatory disorders.
Keywords: cancer biomarker; colorectal cancer; familial adenomatous polyposis; high-resolution mass spectrometry; inflammation; very-long-chain dicarboxylic acid 28:4.
Conflict of interest statement
P.L.W. and L.M.U. have filed a patent regarding VLCDCAs as potential biomarkers for cancer risk and for the utility of analogs/prodrugs as anti-inflammatory and chemopreventive agents.
Figures
Similar articles
-
Endogenous Anti-Inflammatory Very-Long-Chain Dicarboxylic Acids: Potential Chemopreventive Lipids.Metabolites. 2018 Nov 3;8(4):76. doi: 10.3390/metabo8040076. Metabolites. 2018. PMID: 30400281 Free PMC article.
-
Estrogen Receptor β as a Prognostic Marker of Tumor Progression in Colorectal Cancer with Familial Adenomatous Polyposis and Sporadic Polyps.Pathol Oncol Res. 2018 Jul;24(3):533-540. doi: 10.1007/s12253-017-0268-5. Epub 2017 Jul 5. Pathol Oncol Res. 2018. PMID: 28681123
-
The frequency of promoter DNA hypermethylation is decreased in colorectal neoplasms of familial adenomatous polyposis.Oncotarget. 2018 Aug 24;9(66):32653-32666. doi: 10.18632/oncotarget.25987. eCollection 2018 Aug 24. Oncotarget. 2018. PMID: 30220972 Free PMC article.
-
Hereditary colorectal cancer syndromes: familial adenomatous polyposis and lynch syndrome.Surg Clin North Am. 2008 Aug;88(4):819-44, vii. doi: 10.1016/j.suc.2008.04.012. Surg Clin North Am. 2008. PMID: 18672142 Review.
-
The genetic basis of familial adenomatous polyposis and its implications for clinical practice and risk management.Appl Clin Genet. 2015 Apr 16;8:95-107. doi: 10.2147/TACG.S51484. eCollection 2015. Appl Clin Genet. 2015. PMID: 25931827 Free PMC article. Review.
Cited by
-
Plasma Lipid Profile Reveals Plasmalogens as Potential Biomarkers for Colon Cancer Screening.Metabolites. 2020 Jun 25;10(6):262. doi: 10.3390/metabo10060262. Metabolites. 2020. PMID: 32630389 Free PMC article.
-
Dynamics of DHA and EPA supplementation: incorporation into equine plasma, synovial fluid, and surfactant glycerophosphocholines.Metabolomics. 2021 Apr 17;17(5):41. doi: 10.1007/s11306-021-01792-5. Metabolomics. 2021. PMID: 33866431
-
Tryptophan Metabolism as Source of New Prognostic Biomarkers for FAP Patients.Int J Tryptophan Res. 2019 Nov 20;12:1178646919890293. doi: 10.1177/1178646919890293. eCollection 2019. Int J Tryptophan Res. 2019. PMID: 31798304 Free PMC article.
-
Serum Lipidomic Screen Identifies Key Metabolites, Pathways, and Disease Classifiers in Crohn's Disease.Inflamm Bowel Dis. 2023 Jul 5;29(7):1024-1037. doi: 10.1093/ibd/izac281. Inflamm Bowel Dis. 2023. PMID: 36662167 Free PMC article.
References
-
- Brenner H., Tao S. Superior diagnostic performance of faecal immunochemical tests for haemoglobin in a head-to-head comparison with guaiac based faecal occult blood test among 2235 participants of screening colonoscopy. Eur. J. Cancer. 2013;49:3049–3054. doi: 10.1016/j.ejca.2013.04.023. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
