

Cardiac autotransplantation and ex vivo surgical repair of giant left atrium: a case presentation
- PMID: 30563455
- PMCID: PMC6299545
- DOI: 10.1186/s12872-018-0966-2
Cardiac autotransplantation and ex vivo surgical repair of giant left atrium: a case presentation
Abstract
Background: Chronic Mitral Valve disease is strongly associated with Left atrial enlargement; the condition has a high mortality risk. Clinical manifestations include atrial fibrillation, pulmonary hypertension, thromboembolic events, and in cases of Giant Left Atrium (GLA) and a distorted cardiac silhouette. Full sternotomy, conventional open-heart surgery, reductive atrioplasty and atrioventricular valve repair are required to resolve symptoms. However, these procedures can be complicated due to the posterior location of the GLA and concomitant right lateral protrusion. Cardiac autotransplantation is superior under these conditions; it provides improved visual access to the posterior atrial wall and mitral valve, hence, facilitates corrective surgical procedures. We aimed to assess the clinical outcome of patients undergoing cardiac autotransplantation as the primary treatment modality to resolve GLA. Moreover, we evaluated the procedural safety profile and technical feasibility.
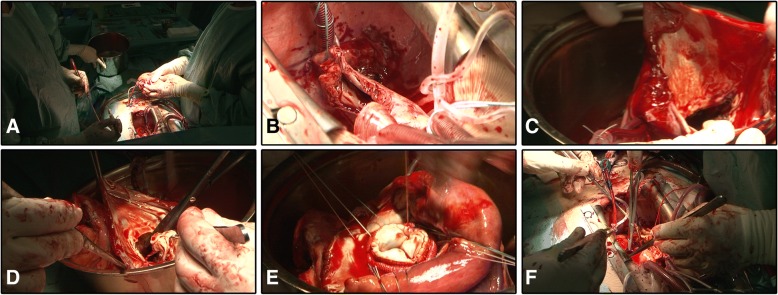
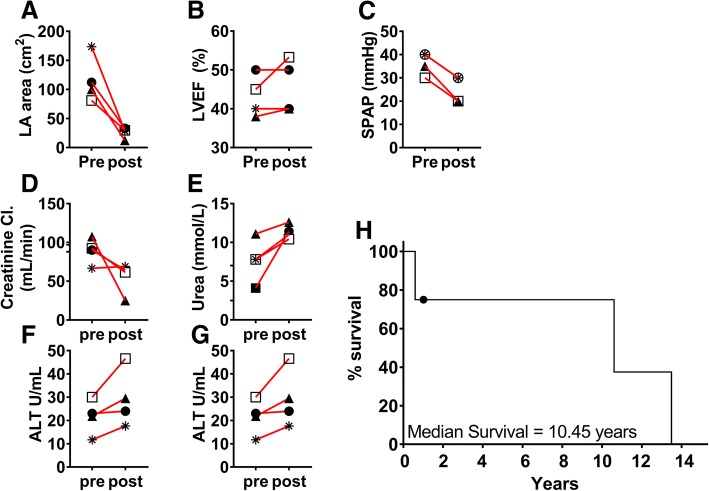
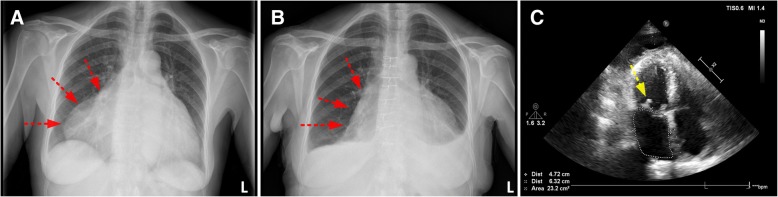
Case presentation: Four patients, mean EuroSCORE II of 23.7% ± 7.7%, presented with heart failure, atrial fibrillation, left atrial diameter > 6.5 cm and a severe distorted cardiac silhouette; X-ray showed prominent right lateral protrusion. We performed cardiac autotransplantation using continuous retrograde perfusion with warm blood supplemented with glucose followed by atrioplasty, atrial plication, valve annuloplasty and valve repair on the explanted beating heart. The surgical approach reduced the left atrial area, mean reduction was - 90.71 cm2 [CI95% -153.3 cm2 to - 28.8 cm2, p = 0.02], and normalized pulmonary arterial pressure, mean decrease - 11.25 mmHg [CI95% -15.23 mmHg to - 7.272 mmHg, p = 0.003]. 3 out of 4 patients experienced an uneventful postoperative course; 2 out of 4 patients experienced a transient return to sinus rhythm following surgery. One was operated on in 2017 and is still in good condition; two other patients survived for more than 10 years; Kaplan-Meier determined median survival is 10.5 years.
Conclusions: Cardiac autotransplantation is an elegant surgical procedure that facilitates the surgical remodelling of Giant Left Atrium. Surgical repair on the ex vivo beating heart, under continuous warm blood perfusion, is a safe procedure applicable also to high-risk patients.
Keywords: Atrial fibrillation; Cardiac autotransplantation; Giant left atrium; Warm blood perfusion.
Conflict of interest statement
Ethics approval and consent to participate
The clinical practice and treatment procedures described in this case series were approved by the ethical committee of the Zan Mitrev Clinic.
Consent for publication
Written and signed informed consent was obtained from patient #4, hospitalised on 28/09/2017, for publication of this case report and any accompanying images. A copy of the signed consent can be submitted upon request for review by the Editor-in-Chief of this journal. The ZMC ethical committee approved the publication of clinical data of the deceased patients #1, #2 and #3 on the condition that full animosity.
Competing interests
Dr. Zan Mitrev is the hospital director at the Zan Mitrev Clinic. The authors of scientific publications receive financial incentives, as a function of the scientific impact of the journal, awarded by the ZMC board.
The ZMC chief scientific officer, R.A. Rosalia, is exempt from any financial incentive system and attests that all clinical and patient data described in this manuscript is devoid of any deliberate falsification or other fraudulent practices. The authors declare no other competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Di Eusanio G, Gregorini R, Mazzola A, Clementi G, Procaccini B, Cavarra F, Taraschi F, Esposito G, Di Nardo W, Di Luzio V. Giant left atrium and mitral valve replacement: risk factor analysis. Eur J Cardiothoracic Surg : official journal of the European Association for Cardio-thoracic Surgery. 1988;2(3):151–159. doi: 10.1016/1010-7940(88)90063-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
