

Identification of subclasses of sepsis that showed different clinical outcomes and responses to amount of fluid resuscitation: a latent profile analysis
- PMID: 30563548
- PMCID: PMC6299613
- DOI: 10.1186/s13054-018-2279-3
Identification of subclasses of sepsis that showed different clinical outcomes and responses to amount of fluid resuscitation: a latent profile analysis
Abstract
Background and objective: Sepsis is a heterogeneous disease and identification of its subclasses may facilitate and optimize clinical management. This study aimed to identify subclasses of sepsis and its responses to different amounts of fluid resuscitation.
Methods: This was a retrospective study conducted in an intensive care unit at a large tertiary care hospital. The patients fulfilling the diagnostic criteria of sepsis from June 1, 2001 to October 31, 2012 were included. Clinical and laboratory variables were used to perform the latent profile analysis (LPA). A multivariable logistic regression model was used to explore the independent association of fluid input and mortality outcome.
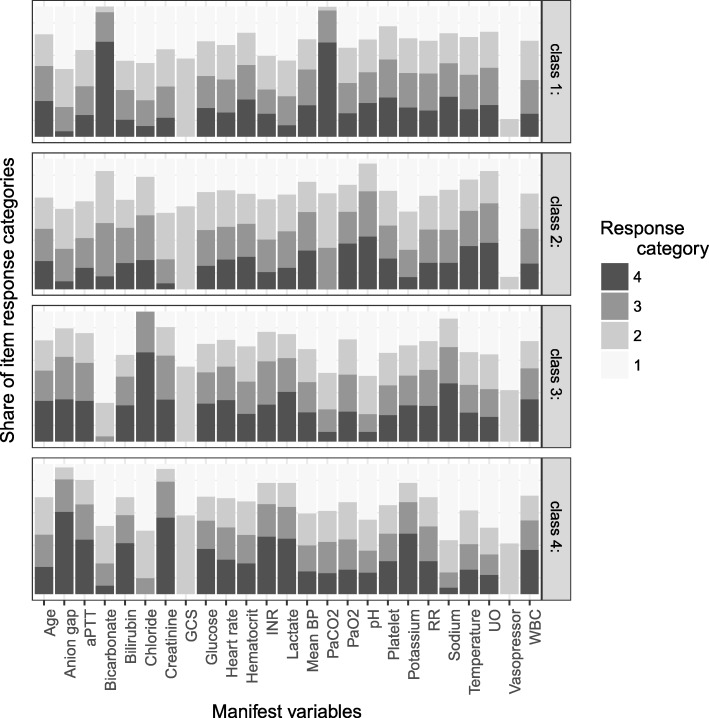
Results: In total, 14,993 patients were included in the study. The LPA identified four subclasses of sepsis: profile 1 was characterized by the lowest mortality rate and having the largest proportion and was considered the baseline type; profile 2 was characterized by respiratory dysfunction; profile 3 was characterized by multiple organ dysfunction (kidney, coagulation, liver, and shock), and profile 4 was characterized by neurological dysfunction. Profile 3 showed the highest mortality rate (45.4%), followed by profile 4 (27.4%), 2 (18.2%), and 1 (16.9%). Overall, the amount of fluid needed for resuscitation was the largest on day 1 (median 5115 mL, interquartile range (IQR) 2662 to 8800 mL) and decreased rapidly on day 2 (median 2140 mL, IQR 900 to 3872 mL). Higher cumulative fluid input in the first 48 h was associated with reduced risk of hospital mortality for profile 3 (odds ratio (OR) 0.89, 95% CI 0.83 to 0.95 for each 1000 mL increase in fluid input) and with increased risk of death for profile 4 (OR 1.20, 95% CI 1.11 to 1.30).
Conclusion: The study identified four subphenotypes of sepsis, which showed different mortality outcomes and responses to fluid resuscitation. Prospective trials are needed to validate our findings.
Keywords: Fluid response; Latent profile analysis; Mortality; Sepsis; Subclass.
Conflict of interest statement
Ethics approval and consent to participate
This study was an analysis of the third-party anonymized databases with pre-existing IRB approval.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
