

Incomplete echocardiographic recovery at 6 months predicts long-term sequelae after intermediate-risk pulmonary embolism. A post-hoc analysis of the Pulmonary Embolism Thrombolysis (PEITHO) trial
- PMID: 30564950
- PMCID: PMC6584226
- DOI: 10.1007/s00392-018-1405-1
Incomplete echocardiographic recovery at 6 months predicts long-term sequelae after intermediate-risk pulmonary embolism. A post-hoc analysis of the Pulmonary Embolism Thrombolysis (PEITHO) trial
Abstract
Introduction: Symptoms and functional limitation are frequently reported by survivors of acute pulmonary embolism (PE). However, current guidelines provide no specific recommendations on which patients should be followed after acute PE, when follow-up should be performed, and which tests it should include. Definition and classification of late PE sequelae are evolving, and their predictors remain to be determined.
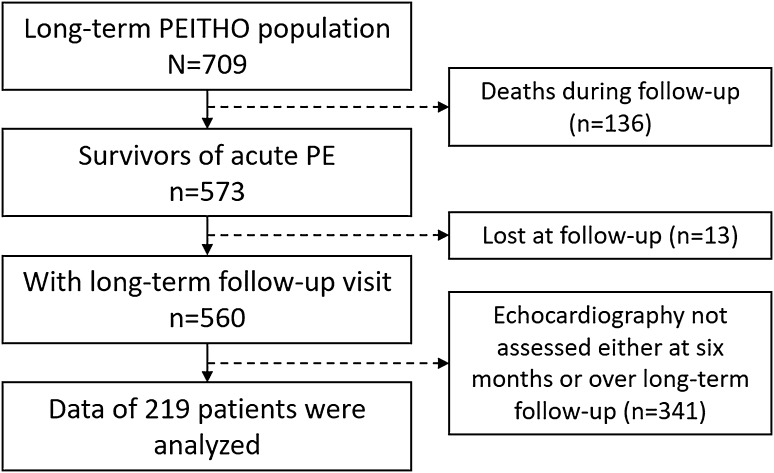
Methods: In a post hoc analysis of the Pulmonary Embolism Thrombolysis (PEITHO) trial, we focused on 219 survivors of acute intermediate-risk PE with clinical and echocardiographic follow-up 6 months after randomisation as well as over the long term (median, 3 years after acute PE). The primary outcome was a composite of (1) confirmed chronic thromboembolic pulmonary hypertension (CTEPH) or (2) 'post-PE impairment' (PPEI), defined by echocardiographic findings indicating an intermediate or high probability of pulmonary hypertension along with New York Heart Association functional class II-IV.
Results: Confirmed CTEPH or PPEI occurred in 29 (13.2%) patients, (6 with CTEPH and 23 with PPEI). A history of chronic heart failure at baseline and incomplete or absent recovery of echocardiographic parameters at 6 months predicted CTEPH or PPEI at long-term follow-up.
Conclusions: CTEPH or PPEI occurs in almost one out of seven patients after acute intermediate-risk PE. Six-month echocardiographic follow-up may be useful for timely detection of late sequelae.
Keywords: Chronic thromboembolic pulmonary hypertension; Post-PE impairment; Pulmonary embolism; Right ventricular dysfunction; Risk stratification.
Conflict of interest statement
SB has received payment for travel accommodation/meeting expenses from Daiichi-Sankyo and Bayer HealthCare. MR has received congress and travel payments from NovoNordisk. DJ has served as an advisor or consultant for Bayer HealthCare Pharmaceuticals. FAK reports research grants from Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Daiichi-Sankyo, MSD and Actelion. OS has received payment for travel accommodation/meeting expenses from Bayer HealthCare, MSD, Actelion, Boehringer Ingelheim, Chiesi; board membership, consultancy and lecture honoraria to his institution from Actelion, Bayer HealthCare, Pfizer—BMS, and Chiesi; and institutional grants from Bayer HealthCare, Actelion, Daiichi-Sankyo, MSD and Portola. SVK reports having received consultancy and lecture honoraria from Bayer HealthCare, Boehringer Ingelheim, Daiichi-Sankyo, and Pfizer—Bristol-Myers Squibb; payment for travel accommodation/ meeting expenses from Bayer HealthCare; and institutional grants from Boehringer Ingelheim, Bayer HealthCare, Daiichi Sankyo, and MSD. Other authors: none reported.
Figures
References
-
- Sista AK, Miller LE, Kahn SR, Kline JA. Persistent right ventricular dysfunction, functional capacity limitation, exercise intolerance, and quality of life impairment following pulmonary embolism: systematic review with meta-analysis. Vasc Med. 2017;22(1):37–43. doi: 10.1177/1358863X16670250. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
