

Newborn screening for severe combined immunodeficiency and T-cell lymphopenia
- PMID: 30565242
- PMCID: PMC6324582
- DOI: 10.1111/imr.12729
Newborn screening for severe combined immunodeficiency and T-cell lymphopenia
Abstract
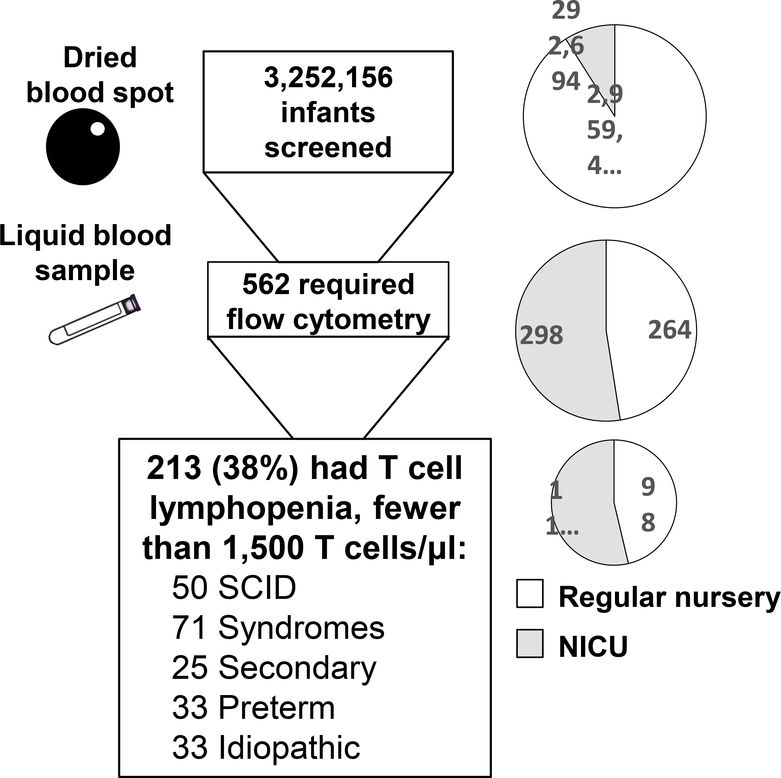
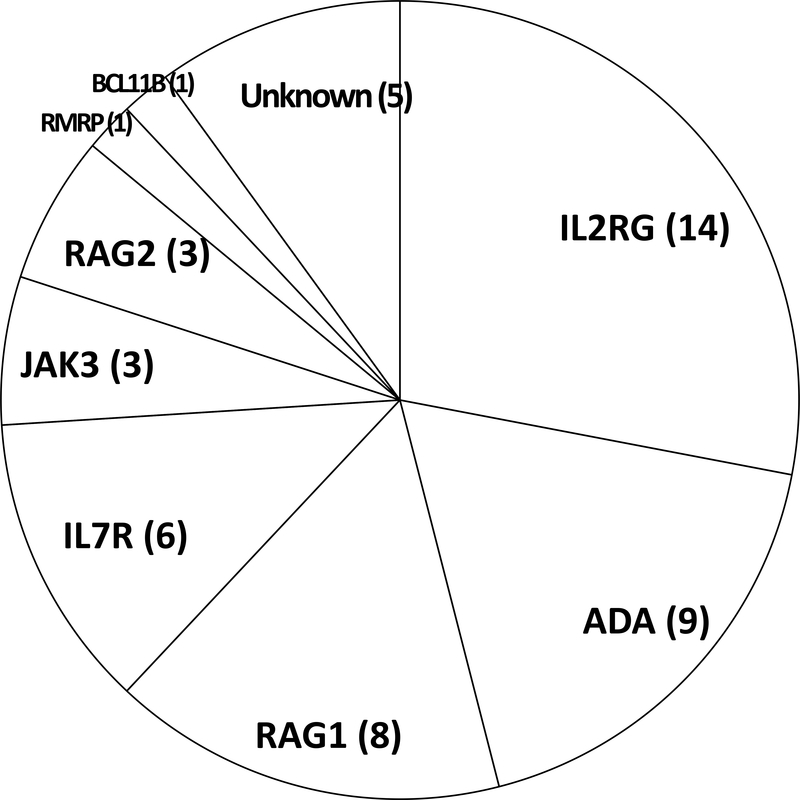
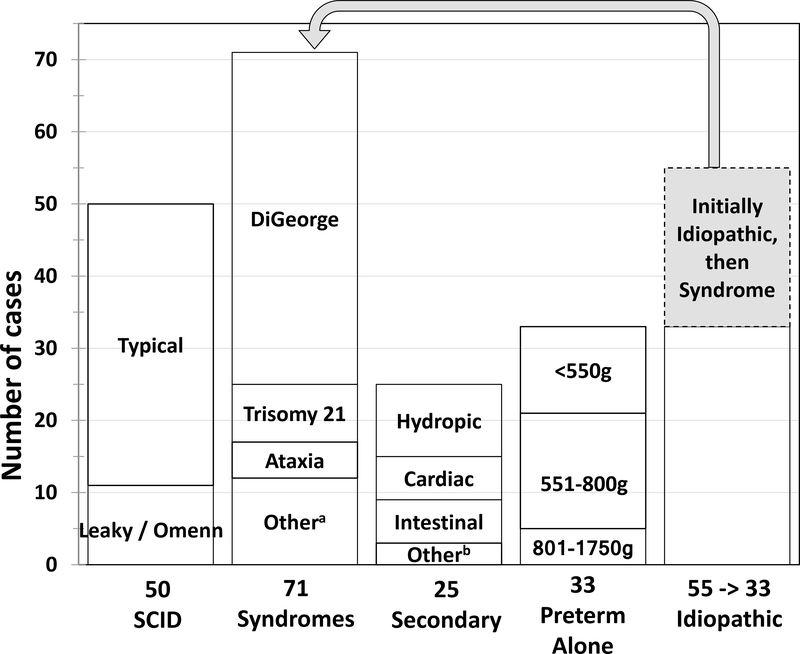
The development of a T cell receptor excision circle (TREC) assay utilizing dried blood spots (DBS) made possible universal newborn screening (NBS) for severe combined immunodeficiency (SCID) as a public health measure. Upon being flagged by an abnormal screening test in a SCID screening program, an infant can receive further diagnostic testing for SCID in the neonatal period, prior to onset of infectious complications, to permit immediate institution of protective measures and definitive, life-saving treatment to establish a functional immune system. SCID screening is now the accepted standard of care in state public health departments across the United States, and it is being adopted in many countries. It has proven effective, with infants having this otherwise inapparent but serious, rare disorder achieving survival and immune reconstitution. In addition to bringing to attention infants with the primary screening target diseases, typical SCID and leaky SCID (due to hypomorphic mutations in known SCID genes), the NBS assay for insufficient TRECs in DBS also reveals infants with non-SCID T lymphopenic conditions. Experience has accumulated regarding the range and limitations of diagnoses of newborns with low TRECs and low T cells. Previously unknown immune defects have been discovered, as well as conditions not formerly recognized to have low T cells in the neonatal period.
Keywords: T cell lymphopenia; T cell receptor excision circle; hematopoietic cell transplantation; newborn screening; primary immunodeficiency; severe combined immunodeficiency.
© 2018 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Dr. Puck reports that her spouse is employed at Invitae, a gene sequencing company; she has no other financial or personal relationships that could be viewed as presenting a potential conflict of interest.
Figures

References
-
- Buckley RH. Molecular defects in human severe combined immunodeficiency and approaches to immune reconstitution. Annu Rev Immunol 2004;22:625–655. - PubMed
-
- Gatti RA, Meuwissen HJ, Allen HD, Hong R, Good RA. Immunological reconstitution of sex-linked lymphopenic immunological deficiency. Lancet 1968;August17;2(7564): 388–389. - PubMed
-
- Buckley RH, Schiff SE, Schiff RI, et al. Hematopoietic stem-cell transplantation for the treatment of severe combined immunodeficiency. N Engl J Med 1999;340:508–516. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
