

Effects of Liraglutide Versus Placebo on Cardiovascular Events in Patients With Type 2 Diabetes Mellitus and Chronic Kidney Disease
- PMID: 30566006
- PMCID: PMC6296845
- DOI: 10.1161/CIRCULATIONAHA.118.036418
Effects of Liraglutide Versus Placebo on Cardiovascular Events in Patients With Type 2 Diabetes Mellitus and Chronic Kidney Disease
Abstract
Background: LEADER trial (Liraglutide Effect and Action in Diabetes: Evaluation of CV Outcome Results) results demonstrated cardiovascular benefits for patients with type 2 diabetes mellitus at high cardiovascular risk on standard of care randomized to liraglutide versus placebo. The effect of glucagon-like peptide-1 receptor agonist liraglutide on cardiovascular events and all-cause mortality in patients with type 2 diabetes mellitus and chronic kidney disease is unknown. Liraglutide's treatment effects in patients with and without kidney disease were analyzed post hoc.
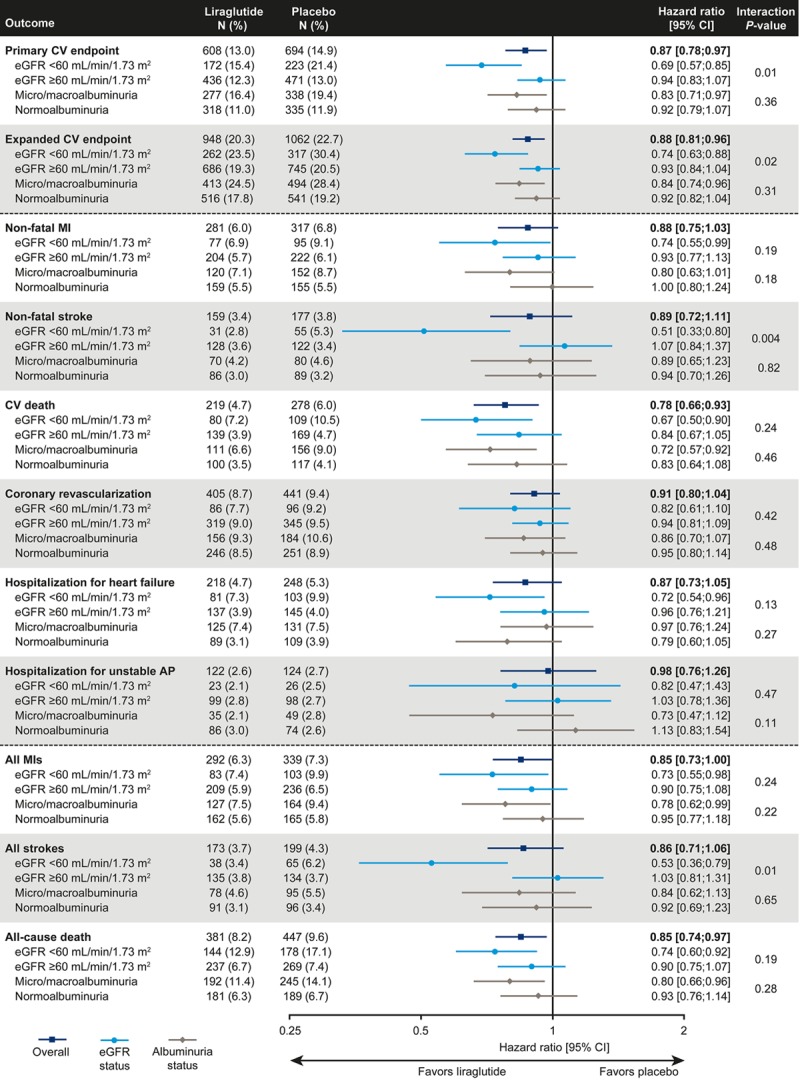
Methods: Patients were randomized (1:1) to liraglutide or placebo, both in addition to standard of care. These analyses assessed outcomes stratified by baseline estimated glomerular filtration rate (eGFR; <60 versus ≥60 mL/min/1.73 m2) and baseline albuminuria. The primary outcome (composite of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) and secondary outcomes, including all-cause mortality and individual components of the primary composite outcome, were analyzed using Cox regression.
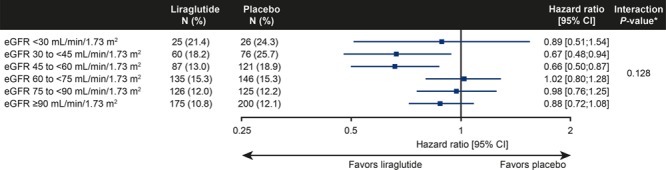
Results: Overall, 2158 and 7182 patients had baseline eGFR <60 or ≥60 mL/min/1.73 m2, respectively. In patients with eGFR <60 mL/min/1.73 m2, risk reduction for the primary composite cardiovascular outcome with liraglutide was greater (hazard ratio [HR], 0.69; 95% CI, 0.57-0.85) versus those with eGFR ≥60 mL/min/1.73 m2 (HR, 0.94; 95% CI, 0.83-1.07; interaction P=0.01). There was no consistent effect modification with liraglutide across finer eGFR subgroups (interaction P=0.13) and when analyzing eGFR as a continuous variable (interaction P=0.61). Risk reductions in those with eGFR <60 versus ≥60 mL/min/1.73 m2 were as follows: for nonfatal myocardial infarction, HR, 0.74; 95% CI, 0.55-0.99 versus HR, 0.93; 95% CI, 0.77-1.13; for nonfatal stroke, HR, 0.51; 95% CI, 0.33-0.80 versus HR, 1.07; 95% CI, 0.84-1.37; for cardiovascular death, HR, 0.67; 95% CI, 0.50-0.90 versus HR, 0.84; 95% CI, 0.67-1.05; for all-cause mortality, HR, 0.74; 95% CI, 0.60-0.92 versus HR, 0.90; 95% CI, 0.75-1.07. Risk reduction for the primary composite cardiovascular outcome was not different for those with versus without baseline albuminuria (HR, 0.83; 95% CI, 0.71-0.97; and HR, 0.92; 95% CI, 0.79-1.07, respectively; interaction P=0.36).
Conclusions: Liraglutide added to standard of care reduced the risk for major cardiovascular events and all-cause mortality in patients with type 2 diabetes mellitus and chronic kidney disease. These results appear to apply across the chronic kidney disease spectrum enrolled.
Clinical trial registration: URL: https://www.clinicaltrials.gov/ . Unique identifier: NCT01179048.
Keywords: LEADER; cardiovascular outcomes; diabetic kidney disease; liraglutide; type 2 diabetes mellitus.
Figures
Comment in
-
Letter by Xie et al Regarding Article, "Effects of Liraglutide Versus Placebo on Cardiovascular Events in Patients With Type 2 Diabetes Mellitus and Chronic Kidney Disease: Results From the LEADER Trial".Circulation. 2019 May 28;139(22):e1015-e1016. doi: 10.1161/CIRCULATIONAHA.118.039071. Epub 2019 May 28. Circulation. 2019. PMID: 31136224 No abstract available.
-
Response by Mann et al to Letter Regarding Article, "Effects of Liraglutide Versus Placebo on Cardiovascular Events in Patients With Type 2 Diabetes Mellitus and Chronic Kidney Disease: Results From the LEADER Trial".Circulation. 2019 May 28;139(22):e1017-e1018. doi: 10.1161/CIRCULATIONAHA.119.040419. Epub 2019 May 28. Circulation. 2019. PMID: 31136226 No abstract available.
References
-
- Muntner P, Anderson A, Charleston J, Chen Z, Ford V, Makos G, O’Connor A, Perumal K, Rahman M, Steigerwalt S, Teal V, Townsend R, Weir M, Wright JT, Jr Chronic Renal Insufficiency Cohort (CRIC) Study Investigators. Hypertension awareness, treatment, and control in adults with CKD: results from the Chronic Renal Insufficiency Cohort (CRIC) study. Am J Kidney Dis. 2010;55:441–451. doi: 10.1053/j.ajkd.2009.09.014. - PMC - PubMed
-
- Ninomiya T, Perkovic V, de Galan BE, Zoungas S, Pillai A, Jardine M, Patel A, Cass A, Neal B, Poulter N, Mogensen CE, Cooper M, Marre M, Williams B, Hamet P, Mancia G, Woodward M, Macmahon S, Chalmers J ADVANCE Collaborative Group. Albuminuria and kidney function independently predict cardiovascular and renal outcomes in diabetes. J Am Soc Nephrol. 2009;20:1813–1821. doi: 10.1681/ASN.2008121270. - PMC - PubMed
-
- van der Velde M, Matsushita K, Coresh J, Astor BC, Woodward M, Levey A, de Jong P, Gansevoort RT, van der Velde M, Matsushita K, Coresh J, Astor BC, Woodward M, Levey AS, de Jong PE, Gansevoort RT, Levey A, El-Nahas M, Eckardt KU, Kasiske BL, Ninomiya T, Chalmers J, Macmahon S, Tonelli M, Hemmelgarn B, Sacks F, Curhan G, Collins AJ, Li S, Chen SC, Hawaii Cohort KP, Lee BJ, Ishani A, Neaton J, Svendsen K, Mann JF, Yusuf S, Teo KK, Gao P, Nelson RG, Knowler WC, Bilo HJ, Joosten H, Kleefstra N, Groenier KH, Auguste P, Veldhuis K, Wang Y, Camarata L, Thomas B, Manley T Chronic Kidney Disease Prognosis Consortium. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality: a collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011;79:1341–1352. doi: 10.1038/ki.2010.536. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
