

Association of Mutations Contributing to Clonal Hematopoiesis With Prognosis in Chronic Ischemic Heart Failure
- PMID: 30566180
- PMCID: PMC6439691
- DOI: 10.1001/jamacardio.2018.3965
Association of Mutations Contributing to Clonal Hematopoiesis With Prognosis in Chronic Ischemic Heart Failure
Abstract
Importance: Somatic mutations causing clonal expansion of hematopoietic cells (clonal hematopoiesis of indeterminate potential [CHIP]) are increased with age and associated with atherosclerosis and inflammation. Age and inflammation are the major risk factors for heart failure, yet the association of CHIP with heart failure in humans is unknown.
Objective: To assess the potential prognostic significance of CHIP in patients with chronic heart failure (CHF) owing to ischemic origin.
Design, setting, and participants: We analyzed bone marrow-derived mononuclear cells from 200 patients with CHF by deep targeted amplicon sequencing to detect the presence of CHIP and associated such with long-term prognosis in patients with CHF at University Hospital Frankfurt, Frankfurt, Germany. Data were analyzed between October 2017 and April 2018.
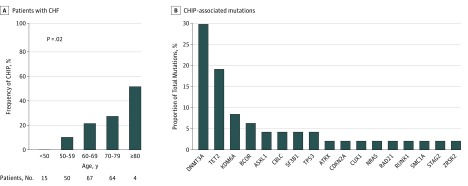
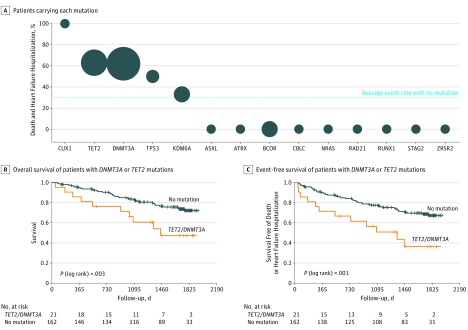
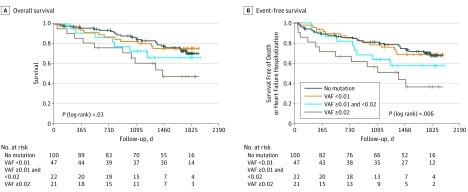
Results: Median age of the patients was 65 years. Forty-seven mutations with a variant allele fraction (VAF) of at least 0.02 were found in 38 of 200 patients with CHF (18.5%). The somatic mutations most commonly occurred in the genes DNMT3A (14 patients), TET2 (9 patients), KDM6A (4 patients), and BCOR (3 patients). Patients with CHIP were older and more frequently had a history of hypertension. During a median follow-up of 4.4 years, a total of 53 patients died, and 23 patients required hospitalization for heart failure. There was a significantly worse long-term clinical outcome for patients with either DNMT3A or TET2 mutations compared with non-CHIP carriers. By multivariable Cox proportional regression analysis, the presence of somatic mutations within TET2 or DNMT3A (HR, 2.1; 95% CI, 1.1-4.0; P = .02, for death combined with heart failure hospitalization) and age (HR, 1.04; 95% CI, 1.01-1.07 per year; P = .005) but not a history of hypertension remained independently associated with adverse outcome. Importantly, there was a significant dose-response association between VAF and clinical outcome.
Conclusions and relevance: Our data suggest that somatic mutations in hematopoietic cells, specifically in the most commonly mutated CHIP driver genes TET2 and DNMT3A, may be significantly associated with the progression and poor prognosis of CHF. Future studies will have to validate our findings in larger cohorts and address whether targeting specific inflammatory pathways may be valuable for precision medicine in patients with CHF carrying specific mutations encoding for CHIP.
Conflict of interest statement
Figures
Comment in
-
CHIPping Away at the Pathogenesis of Heart Failure.JAMA Cardiol. 2019 Jan 1;4(1):5-6. doi: 10.1001/jamacardio.2018.4039. JAMA Cardiol. 2019. PMID: 30566187 No abstract available.
-
Clonal haematopoiesis predicts poor prognosis in heart failure.Nat Rev Cardiol. 2019 Mar;16(3):132. doi: 10.1038/s41569-019-0156-7. Nat Rev Cardiol. 2019. PMID: 30643301 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
