

Long-term Outcomes of Tetralogy of Fallot: A Study From the Pediatric Cardiac Care Consortium
- PMID: 30566184
- PMCID: PMC6439686
- DOI: 10.1001/jamacardio.2018.4255
Long-term Outcomes of Tetralogy of Fallot: A Study From the Pediatric Cardiac Care Consortium
Abstract
Importance: Tetralogy of Fallot (TOF) is a surgically repairable form of cyanotic congenital heart disease. Multicenter data for long-term survival following repair are sparse.
Objective: To evaluate the long-term transplant-free survival of TOF by surgical strategy adjusted for era and patient characteristics.
Design, setting, and participants: Retrospective cohort study enriched with data from the National Death Index and the Organ Procurement and Transplantation Network through 2014. Multicenter cohort from the Pediatric Cardiac Care Consortium (PCCC), a large, US-based clinical registry for interventions for congenital heart disease. The cohort included patients with adequate identifiers for linkage with the National Death Index and the Organ Procurement and Transplantation Network who were enrolled in the PCCC registry between 1982 and 2003 and survived surgical repair of simple TOF. Data were analyzed between September 2015 and April 2018.
Exposures: We examined patient-associated and surgery-associated risk factors affecting survival.
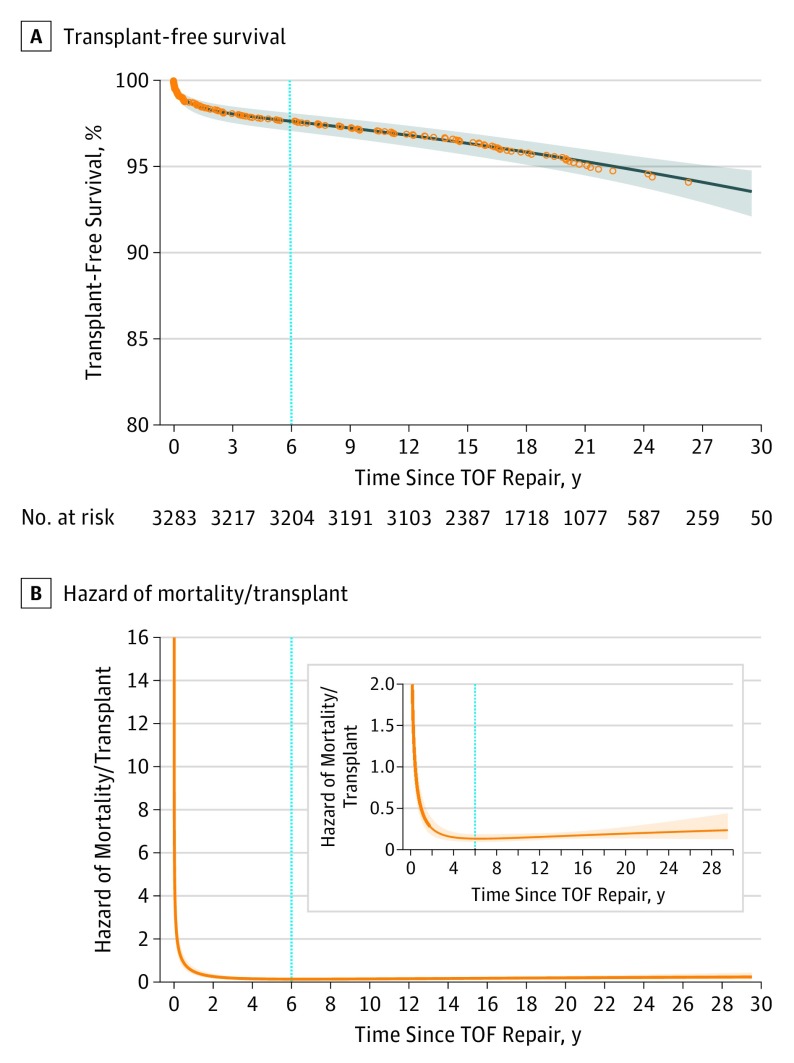
Main outcomes and measures: We analyzed the transplant-free survival during early (<6 years) and late (≥6 years) phase after TOF surgical repair.
Results: Of the 3283 patients who survived repair for simple TOF and met the study's inclusion criteria, 56.4% were male and 43.6% were female. Twenty-five-year survival following TOF repair was 94.5%. Multivariable analysis demonstrated increased risk of early mortality with staged repair (HR, 2.68; 95% CI, 1.59-4.49) and non-valve-sparing operation (HR, 3.76; 95% CI, 1.53-9.19). Presence of a genetic abnormality was associated with increased risk of death both in the early (HR, 3.64; 95% CI, 2.05-6.47) and late postoperative phase (HR, 4.41; 95% CI, 2.62-7.44).
Conclusions and relevance: Long-term survival after simple TOF repair is excellent. Staged repair and non-valve-sparing operations were negatively associated with survival in the early postrepair phase but not the late postrepair phase. These data are important for patients with repaired TOF and their caretakers and may guide surgical strategies for optimizing the long-term outcomes of this population.
Conflict of interest statement
Figures

Comment in
-
Residual Risk After Tetralogy of Fallot Repair.JAMA Cardiol. 2019 Jan 1;4(1):41-42. doi: 10.1001/jamacardio.2018.4331. JAMA Cardiol. 2019. PMID: 30566179 No abstract available.
-
We Can Learn From the Past, but We Must Pave the Future of Congenital Heart Disease Research-Reply.JAMA Cardiol. 2019 Jun 1;4(6):600. doi: 10.1001/jamacardio.2019.1076. JAMA Cardiol. 2019. PMID: 31017614 No abstract available.
-
We Can Learn From the Past, but We Must Pave the Future of Congenital Heart Disease Research.JAMA Cardiol. 2019 Jun 1;4(6):599-600. doi: 10.1001/jamacardio.2019.1066. JAMA Cardiol. 2019. PMID: 31017617 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
