

Muscle atrophy in mechanically-ventilated critically ill children
- PMID: 30566470
- PMCID: PMC6300323
- DOI: 10.1371/journal.pone.0207720
Muscle atrophy in mechanically-ventilated critically ill children
Abstract
Importance: ICU-acquired muscle atrophy occurs commonly and worsens outcomes in adults. The incidence and severity of muscle atrophy in critically ill children are poorly characterized.
Objective: To determine incidence, severity and risk factors for muscle atrophy in critically ill children.
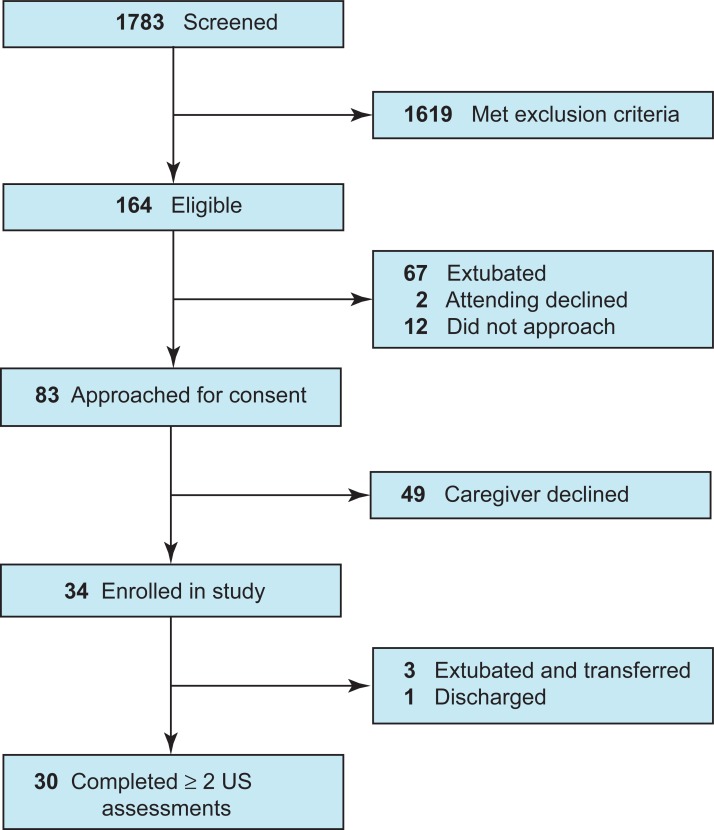
Design, setting and participants: A single-center, prospective cohort study of 34 children receiving invasive mechanical ventilation for ≥48 hours. Patients 1 week- 18 years old with respiratory failure and without preexisting neuromuscular disease or skeletal trauma were recruited from a tertiary Pediatric Intensive Care Unit (PICU) between June 2015 and May 2016. We used serial bedside ultrasound to assess thickness of the diaphragm, biceps brachii/brachialis, quadriceps femoris and tibialis anterior. Serial electrical impedance myography (EIM) was assessed in children >1 year old. Medical records were abstracted from an electronic database.
Exposures: Respiratory failure requiring endotracheal intubation for ≥48 hours.
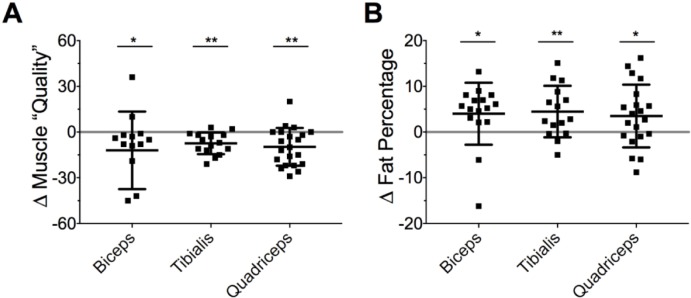
Main outcome and measures: The primary outcome was percent change in muscle thickness. Secondary outcomes were changes in EIM-derived fat percentage and "quality".
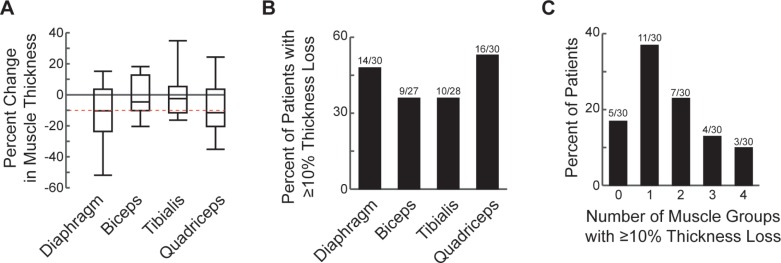
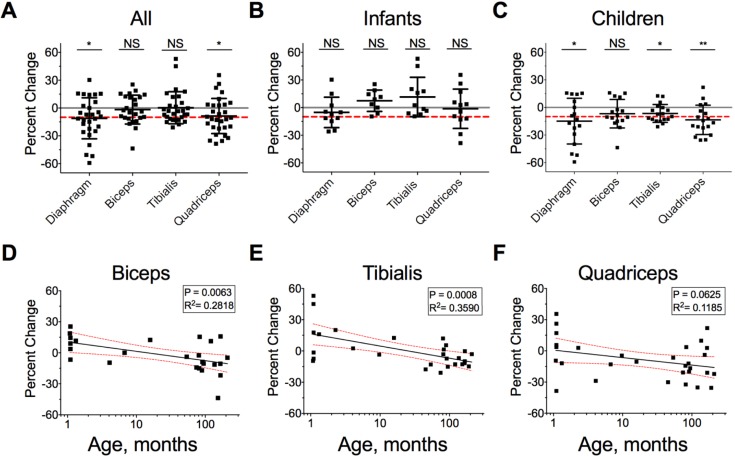
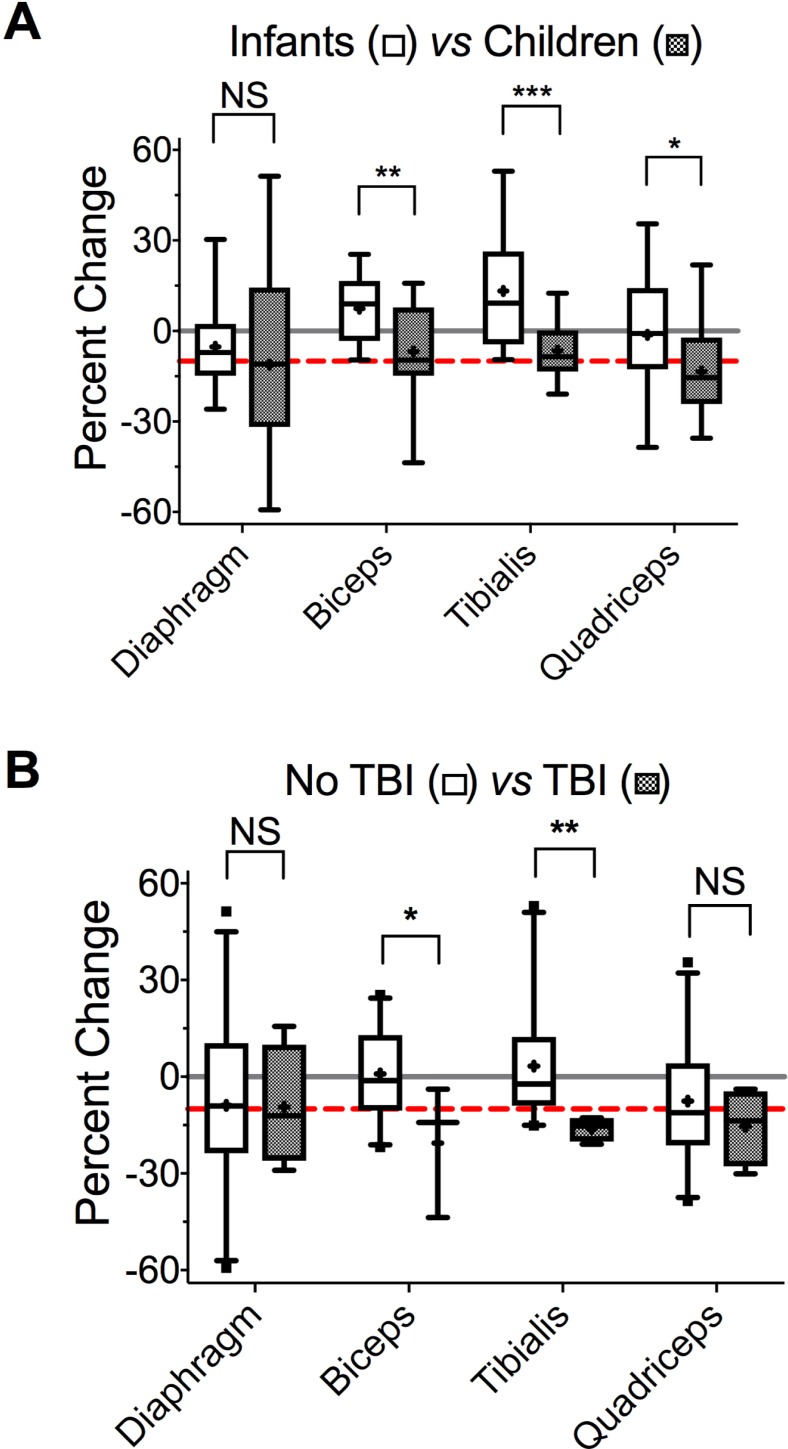
Results: Of 34 enrolled patients, 30 completed ≥2 ultrasound assessments with a median interval of 6 (IQR 6-7) days. Mean age was 5.42 years, with 12 infants <1 year (40%) and 18 children >1 year old (60%). In the entire cohort, diaphragm thickness decreased 11.1% (95%CI, -19.7% to -2.52%) between the first two assessments or 2.2%/day. Quadriceps thickness decreased 8.62% (95%CI, -15.7% to -1.54%) or 1.5%/day. Biceps (-1.71%; 95%CI, -8.15% to 4.73%) and tibialis (0.52%; 95%CI, -5.81% to 3.40%) thicknesses did not change. Among the entire cohort, 47% (14/30) experienced diaphragm atrophy (defined a priori as ≥10% decrease in thickness). Eighty three percent of patients (25/30) experienced atrophy in ≥1 muscle group, and 47% (14/30)-in ≥2 muscle groups. On multivariate linear regression, increasing age and traumatic brain injury (TBI) were associated with greater muscle loss. EIM revealed increased fat percentage and decreased muscle "quality".
Conclusions and relevance: In children receiving invasive mechanical ventilation, diaphragm and other skeletal muscle atrophy is common and rapid. Increasing age and TBI may increase severity of limb muscle atrophy. Prospective studies are required to link muscle atrophy to functional outcomes in critically ill children.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Banwell BL, Mildner RJ, Hassall AC, Becker LE, Vajsar J, Shemie SD. Muscle weakness in critically ill children. Neurology. 2003;61(12):1779–82. Epub 2003/12/25. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
