

Comparative Study
doi: 10.1164/rccm.201808-1435LE.
Mediation Analysis of High Blood Pressure Targets, Arrhythmias, and Shock Mortality
Affiliations
- PMID: 30566846
- PMCID: PMC6423101
- DOI: 10.1164/rccm.201808-1435LE
Item in Clipboard
Comparative Study
Mediation Analysis of High Blood Pressure Targets, Arrhythmias, and Shock Mortality
Am J Respir Crit Care Med.
.
No abstract available
Figures
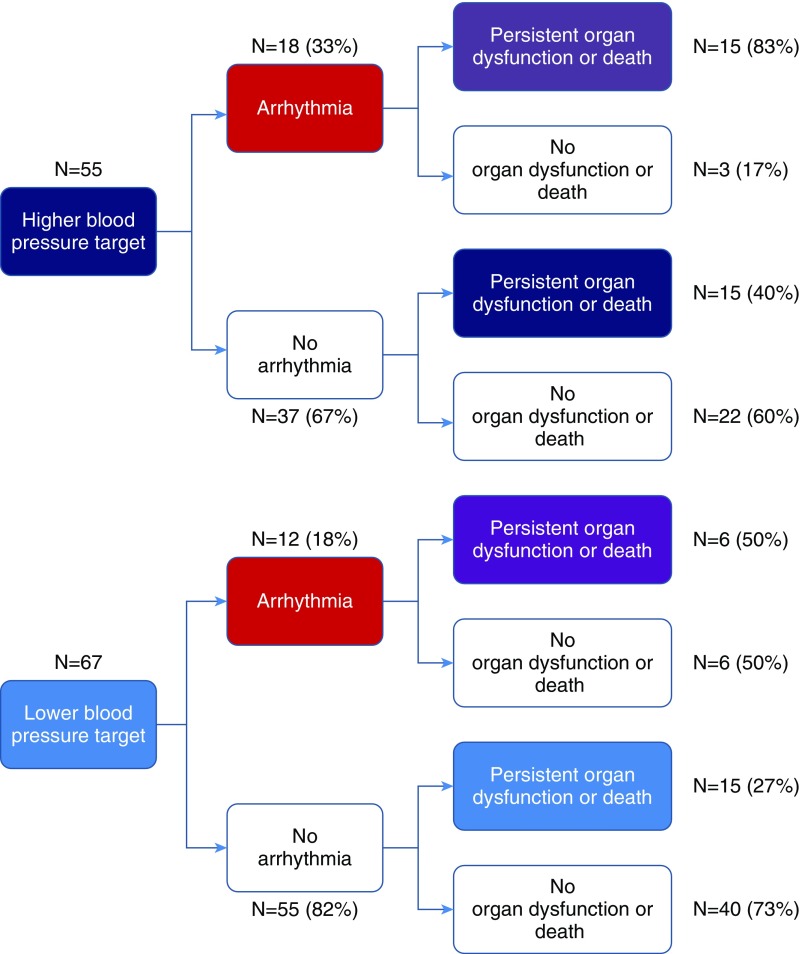
Outcome distributions in the proposed pathways among higher blood pressure targets, arrhythmia, and persistent organ dysfunction or death.
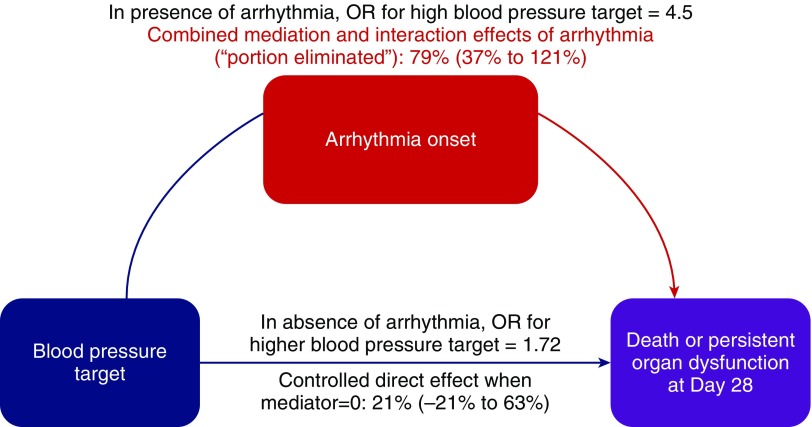
Results of analyses assessing proposed pathways between higher blood pressure targets and persistent organ dysfunction or death that account for effects of arrhythmia through mediation and interaction. Arrhythmias were estimated to account for 79% (95% confidence interval, 37–121%) of the observed effects of higher blood pressure targets on persistent organ dysfunction or death. Effects of higher blood pressure targets on persistent organ dysfunction or death could be decomposed into 1) controlled direct effects 21% (−21% to 63%)—the component not due to mediation by or interaction with arrhythmias, i.e., setting arrhythmia to 0; 2) reference interaction 37% (0.92% to 74%)—the component due to interaction, but not mediation, with arrhythmias; 3) mediated interaction 35% (−0.3% to 70%)—the component due to both mediation by and interaction with arrhythmias; and 4) pure indirect effects 7% (−11% to 24%)—the component due to mediation through arrhythmia alone. OR = odds ratio.
References
-
- Lamontagne F, Day AG, Meade MO, Cook DJ, Guyatt GH, Hylands M, et al. Pooled analysis of higher versus lower blood pressure targets for vasopressor therapy septic and vasodilatory shock. Intensive Care Med. 2018;44:12–21. - PubMed
-
- Asfar P, Meziani F, Hamel J-F, Grelon F, Megarbane B, Anguel N, et al. SEPSISPAM Investigators. High versus low blood-pressure target in patients with septic shock. N Engl J Med. 2014;370:1583–1593. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
