

Postconvulsive central apnea as a biomarker for sudden unexpected death in epilepsy (SUDEP)
- PMID: 30568003
- PMCID: PMC6340388
- DOI: 10.1212/WNL.0000000000006785
Postconvulsive central apnea as a biomarker for sudden unexpected death in epilepsy (SUDEP)
Abstract
Objective: To characterize peri-ictal apnea and postictal asystole in generalized convulsive seizures (GCS) of intractable epilepsy.
Methods: This was a prospective, multicenter epilepsy monitoring study of autonomic and breathing biomarkers of sudden unexpected death in epilepsy (SUDEP) in patients ≥18 years old with intractable epilepsy and monitored GCS. Video-EEG, thoracoabdominal excursions, nasal airflow, capillary oxygen saturation, and ECG were analyzed.
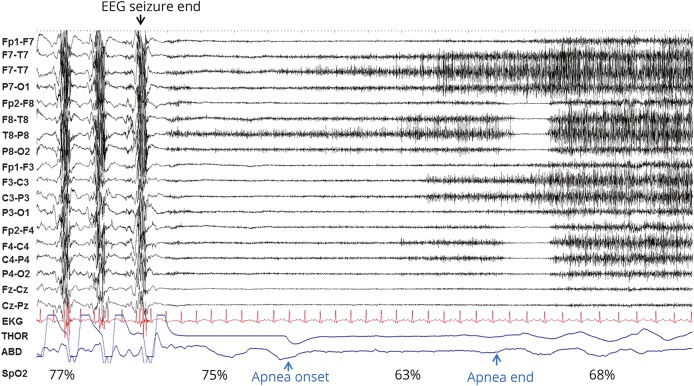
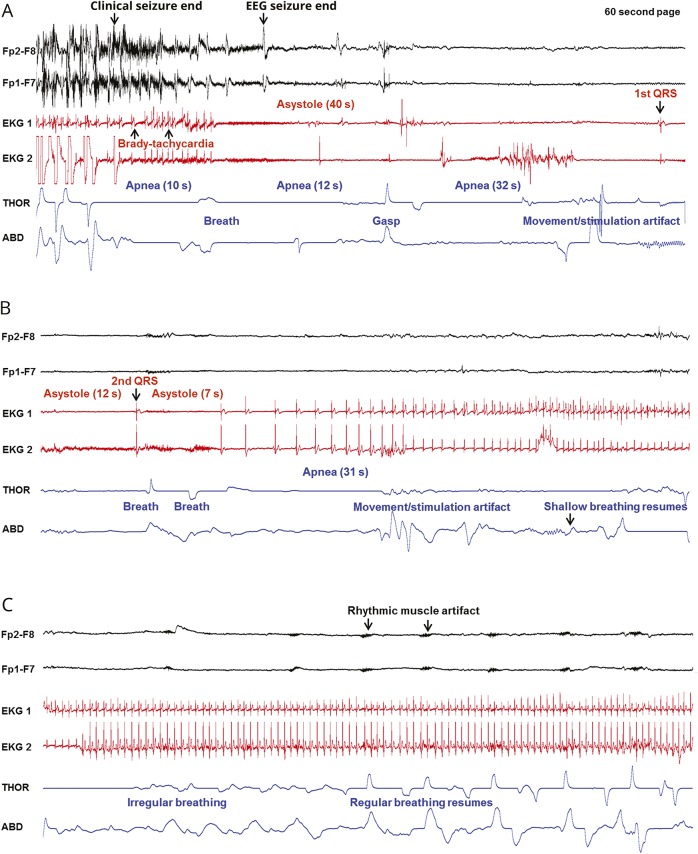
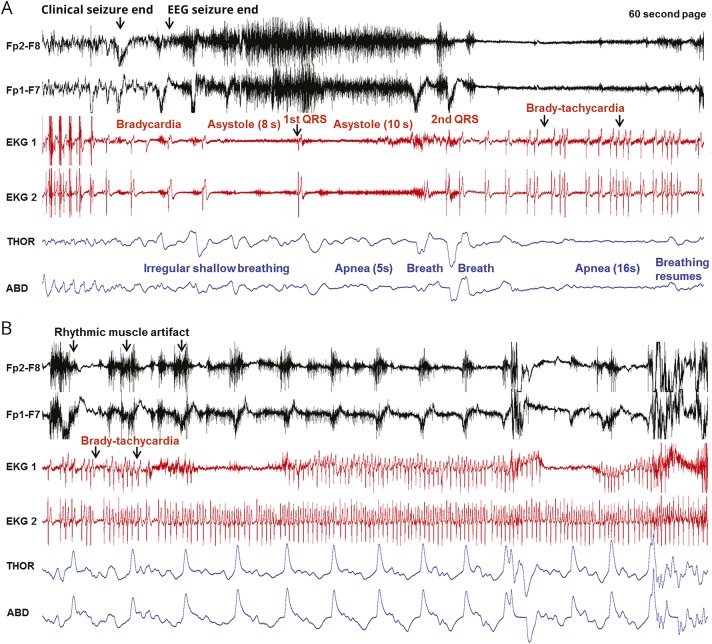
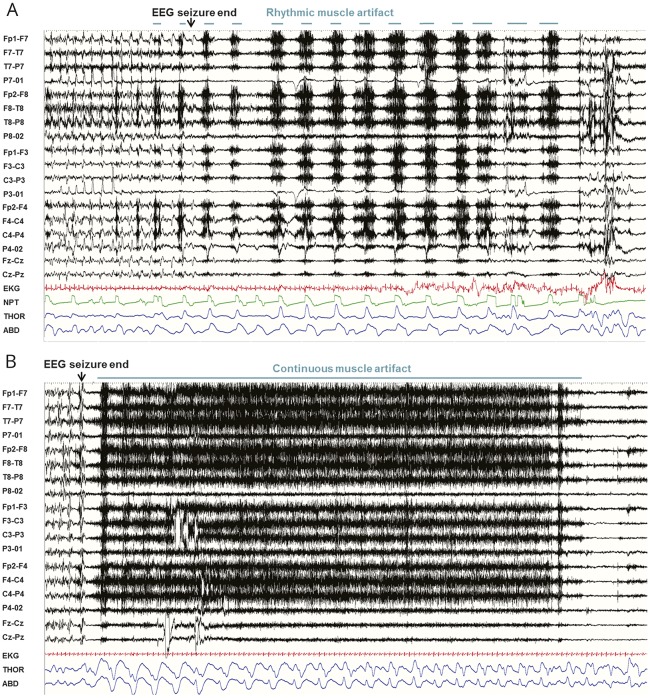
Results: We studied 148 GCS in 87 patients. Nineteen patients had generalized epilepsy; 65 had focal epilepsy; 1 had both; and the epileptogenic zone was unknown in 2. Ictal central apnea (ICA) preceded GCS in 49 of 121 (40.4%) seizures in 23 patients, all with focal epilepsy. Postconvulsive central apnea (PCCA) occurred in 31 of 140 (22.1%) seizures in 22 patients, with generalized, focal, or unknown epileptogenic zones. In 2 patients, PCCA occurred concurrently with asystole (near-SUDEP), with an incidence rate of 10.2 per 1,000 patient-years. One patient with PCCA died of probable SUDEP during follow-up, suggesting a SUDEP incidence rate 5.1 per 1,000 patient-years. No cases of laryngospasm were detected. Rhythmic muscle artifact synchronous with breathing was present in 75 of 147 seizures and related to stertorous breathing (odds ratio 3.856, 95% confidence interval 1.395-10.663, p = 0.009).
Conclusions: PCCA occurred in both focal and generalized epilepsies, suggesting a different pathophysiology from ICA, which occurred only in focal epilepsy. PCCA was seen in 2 near-SUDEP cases and 1 probable SUDEP case, suggesting that this phenomenon may serve as a clinical biomarker of SUDEP. Larger studies are needed to validate this observation. Rhythmic postictal muscle artifact is suggestive of post-GCS breathing effort rather than a specific biomarker of laryngospasm.
© 2018 American Academy of Neurology.
Figures
Comment in
-
Postconvulsive central apnea and asystole: A risk marker for sudden unexpected death in epilepsy (SUDEP)?Neurology. 2019 Jan 15;92(3):115-116. doi: 10.1212/WNL.0000000000006765. Epub 2018 Dec 19. Neurology. 2019. PMID: 30568008 No abstract available.
-
Reader response: Postconvulsive central apnea as a biomarker for sudden unexpected death in epilepsy (SUDEP).Neurology. 2019 Dec 3;93(23):1020-1021. doi: 10.1212/WNL.0000000000008577. Neurology. 2019. PMID: 31792108 No abstract available.
-
Reader response: Postconvulsive central apnea as a biomarker for sudden unexpected death in epilepsy (SUDEP).Neurology. 2019 Dec 3;93(23):1021. doi: 10.1212/WNL.0000000000008586. Neurology. 2019. PMID: 31792109 No abstract available.
-
Author response: Postconvulsive central apnea as a biomarker for sudden unexpected death in epilepsy (SUDEP).Neurology. 2019 Dec 3;93(23):1021-1022. doi: 10.1212/WNL.0000000000008588. Neurology. 2019. PMID: 31792110 No abstract available.
References
-
- Ryvlin P, Nashef L, Lhatoo SD, et al. Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): a retrospective study. Lancet Neurol 2013;12:966–977. - PubMed
-
- Blum AS, Ives JR, Goldberger AL, et al. Oxygen desaturations triggered by partial seizures: implications for cardiopulmonary instability in epilepsy. Epilepsia 2000;41:536–541. - PubMed
-
- Seyal M, Bateman LM, Albertson TE, Lin TC, Li CS. Respiratory changes with seizures in localization-related epilepsy: analysis of periictal hypercapnia and airflow patterns. Epilepsia 2010;51:1359–1364. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous