

The umbilical cord, preeclampsia and the VEGF family
- PMID: 30568515
- PMCID: PMC6276640
- DOI: 10.2147/IJWH.S174734
The umbilical cord, preeclampsia and the VEGF family
Abstract
Introduction: The VEGF family has been identified as abnormal in preeclampsia (PE). Hypertensive disorders of pregnancy (HDP) are major contributors to maternal and neonatal morbidity and mortality worldwide; likewise, umbilical cord anatomical abnormalities (UCAA) are linked to poor neonatal outcomes. Based on the relationship described between PE and UCAA and the role of the VEGF family in PE, this study explored VEGF expression in placental and UC tissued from patients with PE and with UCAA.
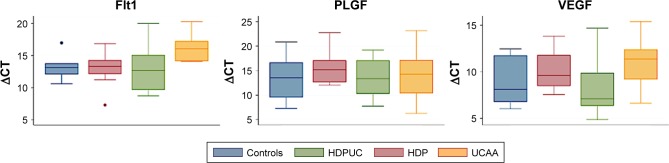
Methods: We performed an observational, analytical study on placentas, comparing protein and mRNA expression in four groups: patients with PE, patients with UC abnormalities, patients with both, and patients with none of them. Using immunohistochemistry, we studied VEGF A, VEGF R1 (FLT1), MMP1, and PLGF. With quantitative reverse transcription polymerase chain reaction we described mRNA expression of PLGF, VEGF and sFLT1, and sFLT1/PLGF ratio.
Results: Forty newborns were included. Sixty-seven percent of mothers and 45% of newborns developed no complications. Immunohistochemistry was performed on UC and placental disc paraffin-embedded tissue; in the latter, the mRNA of the VEGF family was also measured. Statistically significant differences were observed among different expressions in both HDP and UCAA groups. Interestingly, the UCAA group exhibited lower levels of sFLT1 and VEGF-A in comparison with other groups, with significant P-value for sFLT1 (P=0000.1).
Conclusion: The origin of UCAA abnormalities and their relation with HDP are still unknown. VEGF family alterations could be involved in both. This study provides the first approach related to molecules linked to UCAA.
Keywords: PLGF; VEGF; preeclampsia; sFLT1; stillbirth; umbilical cord.
Conflict of interest statement
Disclosure None of the authors has any potential or actual interests relevant to the topics discussed in this manuscript. The authors report no conflicts of interest in this work.
Figures







References
-
- US Preventive Services Task Force. Bibbins-Domingo K, Grossman DC, et al. Screening for preeclampsia: US preventive services task force recommendation statement. JAMA. 2017;317(16):1661–1667. - PubMed
-
- Foo L, Tay J, Lees CC, McEniery CM, Wilkinson IB. Hypertension in pregnancy: natural history and treatment options. Curr Hypertens Rep. 2015;17(5):36. - PubMed
-
- Shennan AH, Green M, Chappell LC. Maternal deaths in the UK: pre-eclampsia deaths are avoidable. Lancet. 2017;389(10069):582–584. - PubMed
-
- Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet. 2010;376(9741):631–644. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
