

Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: A Review of the Literature
- PMID: 30568655
- PMCID: PMC6290896
- DOI: 10.3389/fimmu.2018.02802
Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: A Review of the Literature
Abstract
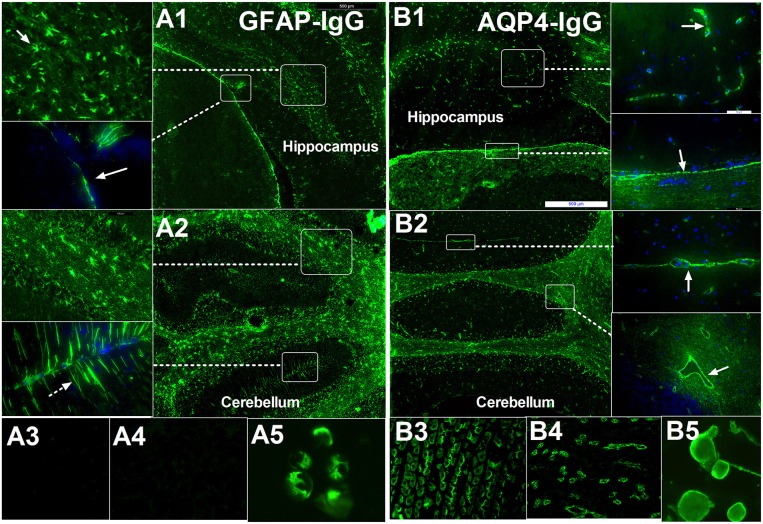
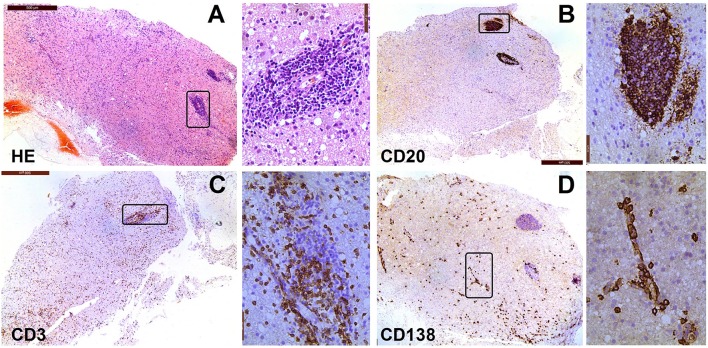
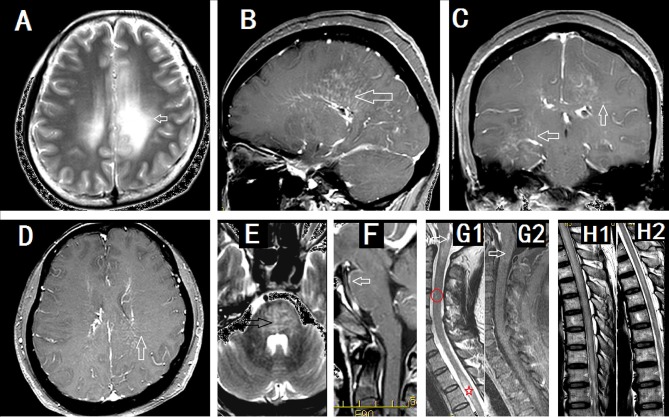
Autoimmune glial fibrillary acidic protein (GFAP) astrocytopathy is an autoimmune disease of the nervous system first defined in 2016. GFAP autoantibody, especially IgG that binds to GFAPα, has been reported in the cerebrospinal fluid (CSF) and serum of patients with GFAP astrocytopathy. The positive predictive value of GFAP antibody in the CSF is higher than in the serum. Tissue-based assay (TBA) and cell-based assay (CBA) are both recommended methods for the detection of GFAP antibody. GFAP astrocytopathy is accompanied by neoplasms, but the relationship between virus infection and GFAP astrocytopathy is unclear. GFAP antibody itself does not induce pathological changes; it is only a biomarker for the process of immune inflammation. The pathology of GFAP astrocytopathy in humans is heterogeneous. GFAP astrocytopathy is commonly diagnosed in individuals over 40 years old and most patients have an acute or subacute onset. Clinical manifestations include fever, headache, encephalopathy, involuntary movement, myelitis, and abnormal vision. Lesions involve the subcortical white matter, basal ganglia, hypothalamus, brainstem, cerebellum, and spinal cord. The characteristic MRI feature is brain linear perivascular radial gadolinium enhancement in the white matter perpendicular to the ventricle. Currently, there are no uniform diagnostic criteria or consensus for GFAP astrocytopathy and coexisting neural autoantibodies detected in the same patient make the diagnosis difficult. A standard treatment regimen is yet to be developed. Most GFAP astrocytopathy patients respond well to steroid therapy although some patients are prone to relapse or even die.
Keywords: antibody; astrocyte; astrocytopathy; glial fibrillary acidic protein; meningoencephalitis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous