

Clinical and Epidemiologic Profiles for Identifying Norovirus in Acute Gastroenteritis Outbreak Investigations
- PMID: 30568985
- PMCID: PMC5892141
- DOI: 10.1093/ofid/ofy049
Clinical and Epidemiologic Profiles for Identifying Norovirus in Acute Gastroenteritis Outbreak Investigations
Abstract
Background: Noroviruses are the leading cause of acute gastroenteritis (AGE) outbreaks in the United States. However, outbreaks attributed to norovirus often lack confirmation by diagnostic testing. Clinical and epidemiologic profiles, such as the Kaplan criteria (vomiting in >50% cases, mean incubation period of 24-48 hours, mean duration of illness for 12-60 hours, and negative bacterial stool culture), have been used to distinguish norovirus outbreaks from those caused by bacteria.
Methods: Kaplan criteria were evaluated among 10 023 outbreaks reported to the National Outbreak Reporting System (NORS) during 2009-2012. An alternate profile for distinguishing norovirus outbreaks from outbreaks caused by nonviral etiologies was identified using classification and regression tree (CART) modeling. Performance of the Kaplan criteria and alternate profile were compared among laboratory-confirmed outbreaks.
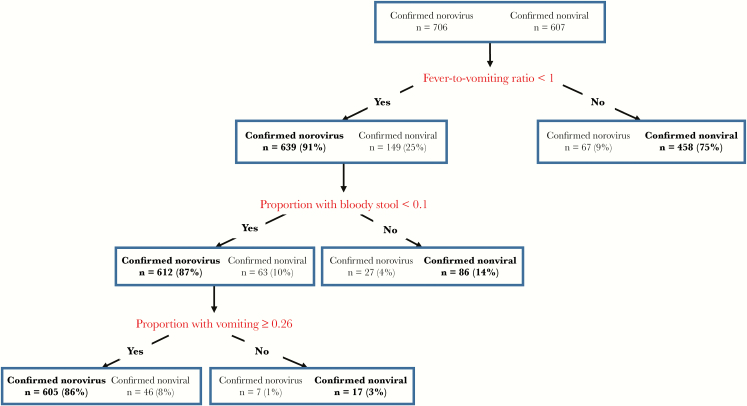
Results: The Kaplan criteria were 63.9% sensitive and 100% specific in discriminating norovirus from nonviral outbreaks, but only 3.3% of norovirus and 1.2% of nonviral outbreaks reported all criteria. Clinical and epidemiologic characteristics identified with CART modeling (ratio of proportion of cases with fever to the proportion of cases with vomiting <1, proportion of cases with bloody stool <0.1, proportion of cases with vomiting ≥0.26) were 85.7% sensitive and 92.4% specific for distinguishing norovirus from nonviral outbreaks and were applicable to more than 8 times as many outbreaks compared with the Kaplan criteria.
Conclusions: Compared with the Kaplan criteria, the CART-derived profile had higher sensitivity and broader application in reported AGE outbreaks. Thus, this alternate profile may provide a more useful tool for identifying norovirus during outbreak investigations.
Keywords: CART modeling; Kaplan criteria; acute gastroenteritis; clinical and epidemiologic profiles; norovirus; outbreaks.
Figures
References
-
- Hall AJ, Vinjé J, Lopman B, et al. Updated Norovirus Outbreak Management and Disease Prevention Guidelines. MMWR Recomm Rep 2011; 60:1–15. - PubMed
LinkOut - more resources
Full Text Sources
