

Healthcare Costs of Smokers Using Varenicline Versus Nicotine-Replacement Therapy Patch in the United States: Evidence from Real-World Practice
- PMID: 30569324
- PMCID: PMC6824348
- DOI: 10.1007/s12325-018-0858-y
Healthcare Costs of Smokers Using Varenicline Versus Nicotine-Replacement Therapy Patch in the United States: Evidence from Real-World Practice
Abstract
Introduction: Varenicline (VAR) is an effective smoking-cessation therapy compared to the commonly used nicotine-replacement therapy patch (NRT-P). However, comparative real-world evidence on smoking-cessation therapies is limited, especially for economic outcomes.
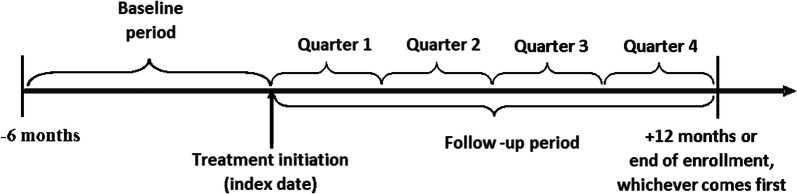
Methods: Using national claims databases (2012-2016) in the United States (US), adults initiating VAR or NRT-P without use of any other smoking-cessation products were followed for up to 1 year on a quarterly basis. Outcomes included smoking-attributable (SA) (cardiovascular, diabetes, pulmonary diseases, and smoking cessation) and all-cause costs (2017 US dollars). Adjusted mean costs were estimated from multivariable regressions, with baseline characteristics and propensity scores as covariates. Annual adjusted costs were calculated from quarterly averages.
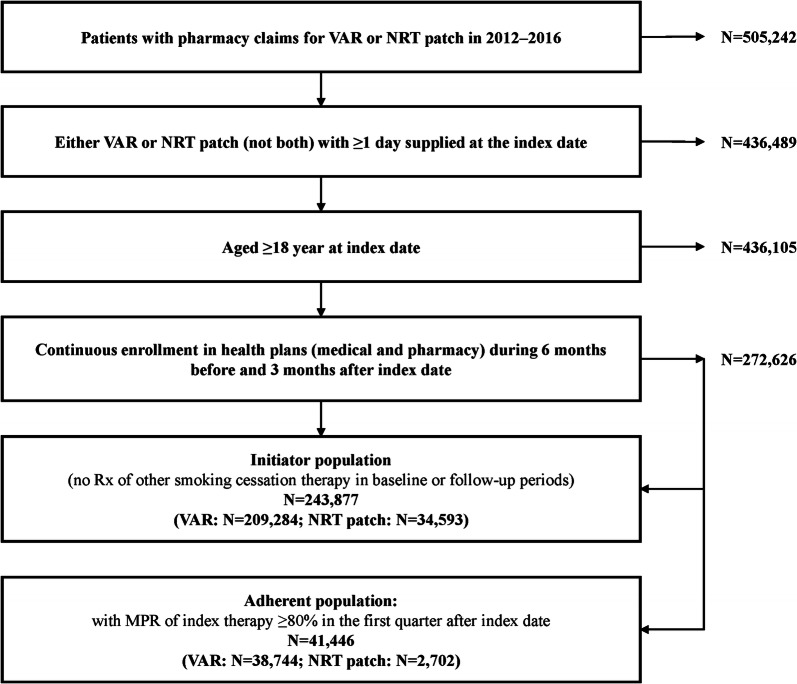
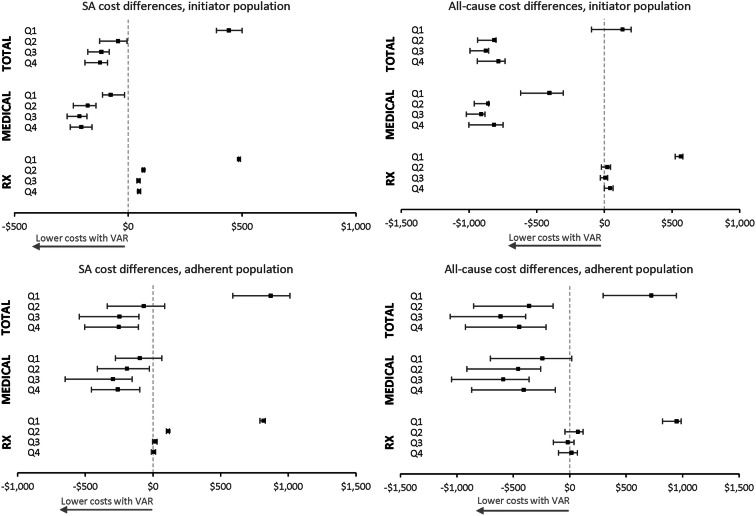
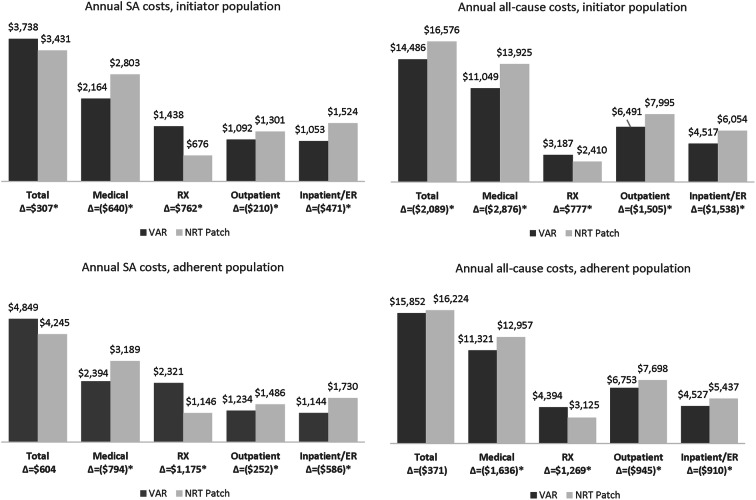
Results: The VAR cohort (n = 209,284) was younger (mean age 46.7 vs. 49.0 years) and had fewer comorbidities [mean Charlson Comorbidity Index (CCI): 0.8 vs. 1.6] than the NRT-P cohort (n = 34,593). After adjustment, VAR cohort had lower SA and all-cause medical costs than NRT-P cohort in Quarters 1-4 (Q1-Q4) of follow-up, and had lower SA and all-cause total costs in Q2-Q4. Annually, VAR cohort had higher SA total costs ($307) and lower all-cause costs (- $2089) than NRT-P cohort. Annual medical costs were lower in VAR cohort (- $640 for SA and - $2876 for all-cause), and pharmacy costs were higher ($762 for SA and $777 for all-cause). In adherent patients (VAR: n = 38,744; NRT-P: n = 2702), VAR patients had lower annual medical costs (- $794 for SA and - $1636 for all-cause) and higher pharmacy costs ($1175 for SA and $1269 for all-cause); differences in SA and all-cause total costs were not statistically significant between treatment groups.
Conclusions: Lower SA and all-cause medical costs associated with the use of VAR versus NRT-P resulted in savings in all-cause total costs and, among adherent patients, potentially offset the high pharmacy costs of VAR.
Funding: Pfizer, Inc.
Keywords: Healthcare costs; Real-world evidence; Varenicline.
Conflict of interest statement
L. Lee is employed by and owns stock in Pfizer. M Bruno is employed by and owns stock in Pfizer. B. Emir is employed by and owns stock in Pfizer. N. Marchant is employed by and owns stock in Pfizer. P. Park is employed by and owns stock in Pfizer. Q. Li is employed by Evidera. S. Shah is employed by Evidera. B. Murphy is employed by Evidera. M. Reynolds is employed by Evidera. Evidera (a division of PPD) provides consulting and other research services to pharmaceutical, device, and related organizations. In their salaried positions, they work with a variety of companies and organizations, and are precluded from receiving payment or honoraria directly for services rendered. Evidera received funding from Pfizer to participate in the study and for the development of this manuscript.
Figures
Similar articles
-
Comparative Effectiveness of Varenicline and Nicotine Replacement Therapy for Smoking Cessation in Older and Younger Smokers: A Prospective Cohort in Taiwan.Nicotine Tob Res. 2019 Jan 4;21(2):149-155. doi: 10.1093/ntr/ntx275. Nicotine Tob Res. 2019. PMID: 29294121 Free PMC article.
-
Smokers with opioid use disorder may have worse drug use outcomes after varenicline than nicotine replacement.J Subst Abuse Treat. 2019 Sep;104:22-27. doi: 10.1016/j.jsat.2019.06.005. Epub 2019 Jun 10. J Subst Abuse Treat. 2019. PMID: 31370981 Free PMC article. Clinical Trial.
-
Cost-effectiveness of varenicline versus bupropion, nicotine-replacement therapy, and unaided cessation in Greece.Clin Ther. 2012 Aug;34(8):1803-14. doi: 10.1016/j.clinthera.2012.07.002. Epub 2012 Jul 20. Clin Ther. 2012. PMID: 22818870
-
[Pharmacotherapy for Smoking Cessation During Pregnancy - CNGOF-SFT Expert Report and Guidelines for Smoking Management During Pregnancy].Gynecol Obstet Fertil Senol. 2020 Jul-Aug;48(7-8):604-611. doi: 10.1016/j.gofs.2020.03.030. Epub 2020 Apr 1. Gynecol Obstet Fertil Senol. 2020. PMID: 32247100 Review. French.
-
Different doses, durations and modes of delivery of nicotine replacement therapy for smoking cessation.Cochrane Database Syst Rev. 2019 Apr 18;4(4):CD013308. doi: 10.1002/14651858.CD013308. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2023 Jun 19;6:CD013308. doi: 10.1002/14651858.CD013308.pub2. PMID: 30997928 Free PMC article. Updated.
Cited by
-
Short-term effects of national smoking cessation service on smoking-related disease prevalence and healthcare costs: Experience from the National Health Insurance Service Smoking Cessation Intervention Program in Korea.Tob Induc Dis. 2023 Aug 24;21:107. doi: 10.18332/tid/169654. eCollection 2023. Tob Induc Dis. 2023. PMID: 37637229 Free PMC article.
-
Varenicline and Nicotine Replacement Use Associated With US Food and Drug Administration Drug Safety Communications.JAMA Netw Open. 2019 Sep 4;2(9):e1910626. doi: 10.1001/jamanetworkopen.2019.10626. JAMA Netw Open. 2019. PMID: 31483473 Free PMC article.
-
Primary care-based smoking cessation treatment and subsequent healthcare service utilisation: a matched cohort study of smokers using linked administrative healthcare data.Tob Control. 2023 Jan;32(1):72-79. doi: 10.1136/tobaccocontrol-2021-056522. Epub 2021 Jun 3. Tob Control. 2023. PMID: 34083493 Free PMC article.
-
Association Between Smoking Cessation Treatment and Healthcare Costs in a Single-Payer Public Healthcare System.Nicotine Tob Res. 2023 Jan 1;25(1):86-93. doi: 10.1093/ntr/ntac166. Nicotine Tob Res. 2023. PMID: 35792868 Free PMC article.
-
The Relative Value of Anti-Obesity Medications Compared to Similar Therapies.Clinicoecon Outcomes Res. 2023 Jan 26;15:51-62. doi: 10.2147/CEOR.S392276. eCollection 2023. Clinicoecon Outcomes Res. 2023. PMID: 36726966 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Current Cigarette Smoking among Adults in the United States 2016.
-
- US Department of Health and Human Services. The health consequences of smoking—50 years of progress: a report of the Surgeon General: full report. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health, Office on Smoking and Health; 2014.
-
- US Department of Health and Human Services. How Tobacco Smoke Causes Disease. The Biology and Behavioral Basis for Smoking-Attributable Disease: A report of the Surgeon General. Atlanta, GA, USA; 2010. - PubMed
-
- US Department of Health and Human Services. The health consequences of smoking—50 years of progress: a report of the Surgeon General: full report 2014.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
