

Review
doi: 10.1007/s12350-018-01552-4.
Epub 2018 Dec 19.
State-of-the-art radionuclide imaging in cardiac transthyretin amyloidosis
Affiliations
- PMID: 30569412
- PMCID: PMC6541031
- DOI: 10.1007/s12350-018-01552-4
Item in Clipboard
Review
State-of-the-art radionuclide imaging in cardiac transthyretin amyloidosis
J Nucl Cardiol.
2019 Feb.
Abstract
Cardiac amyloidosis, once considered untreatable, is now gaining well-deserved attention due to advances in imaging and the recent approval of targeted breakthrough therapies. In this paper, we discuss the role of radionuclide imaging in the evaluation and management of patients with the most common form of amyloidosis-cardiac transthyretin amyloidosis (ATTR). We provide a comprehensive summary of the literature interspersed with our institutional experience as appropriate, to deliver our perspective.
Keywords: Amyloid heart disease; PET; SPECT; modalities; molecular imaging.
Figures
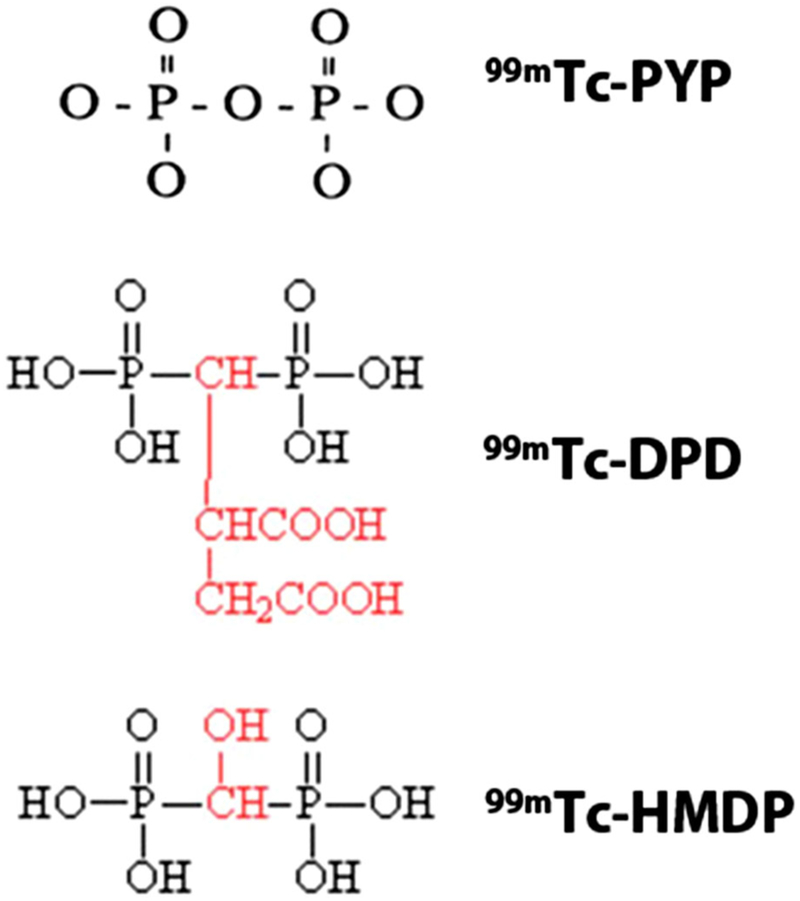
Bone avid SPECT radiotracers for imaging cardiac amyloidosis. 99mTc pyrophosphate (PYP), 3,3-diphosphono-1,2-propanedicarboxylic acid (DPD), and hydroxymethylene diphosphonate (HMDP) have been used for imaging ATTR cardiac amyloidosis. These bone avid SPECT tracers show greater uptake in ATTR cardiac amyloidosis. Images adapted from package insert of 99mTc PYP, and from Human Health Campus, IAEA.
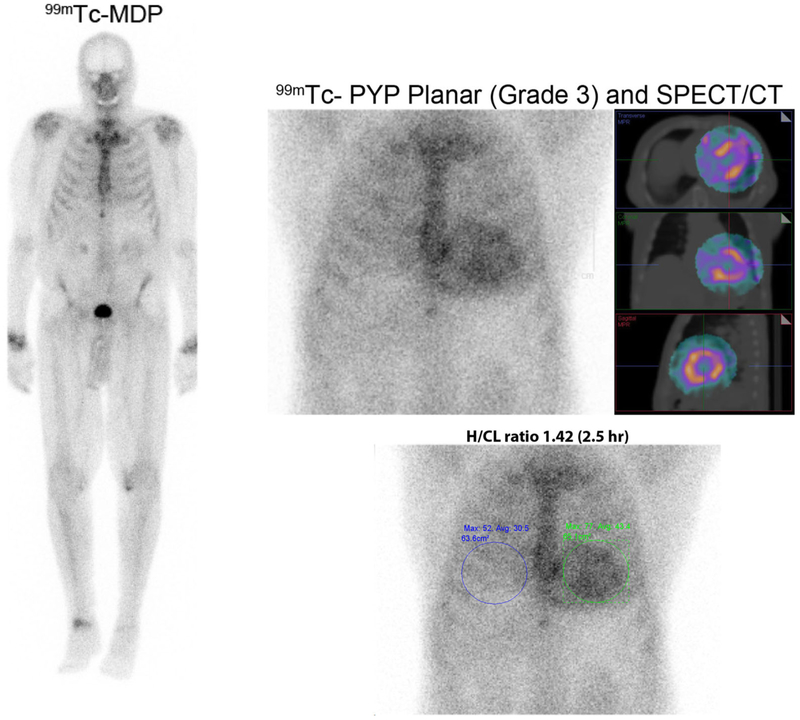
99mTc-MDP and 99mTc-PYP images in cardiac ATTR amyloidosis. Images of an 86-year-old man with prostate cancer and a 99mTc-MDP scan showing no myocardial radiotracer uptake. He presented a month later with heart failure, and echocardiography revealed classic features of cardiac amyloidosis. A clonal abnormality was excluded by serum and urine immunofixation, and serum-free light chain levels. A 99mTc-PYP scan was performed using chest planar and SPECT imaging 2.5 hours after injection of radiotracer; Grade 3 myocardial uptake on 99mTc-PYP planar, and SPECT with a heart-to-contralateral ratio of 1.42 on planar images (≥ 1.3 abnormal for late images) diagnosed cardiac ATTR amyloidosis.
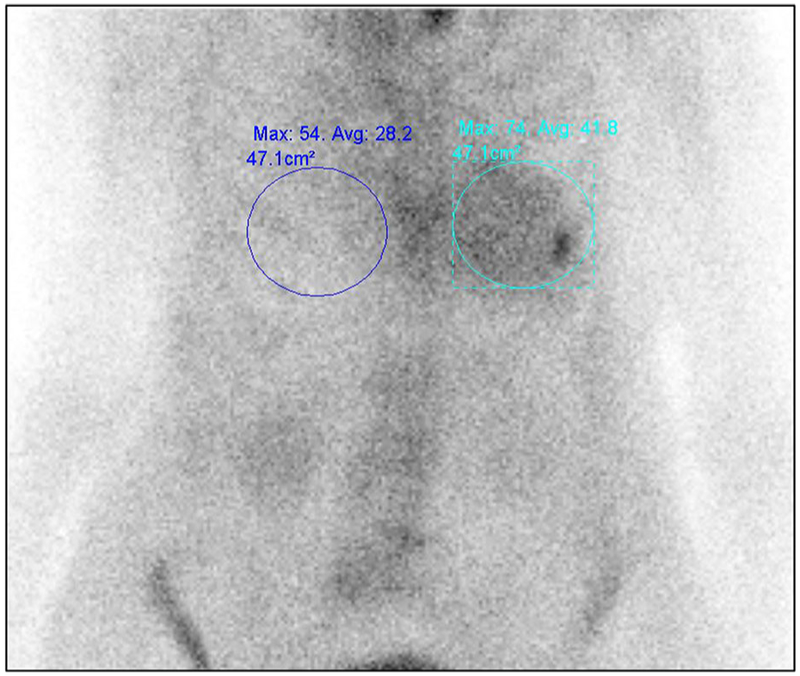
Planar 99mTc-PYP imaging limited by overlying rib uptake. When evaluating the heart-to-contralateral lung uptake ratio (H/CL), care must be taken to avoid increase the bone activity overlying the myocardial region. In this chest planar 99mTc-PYP image, focally increased radiotracer uptake in the left chest is due to a recent rib fracture.
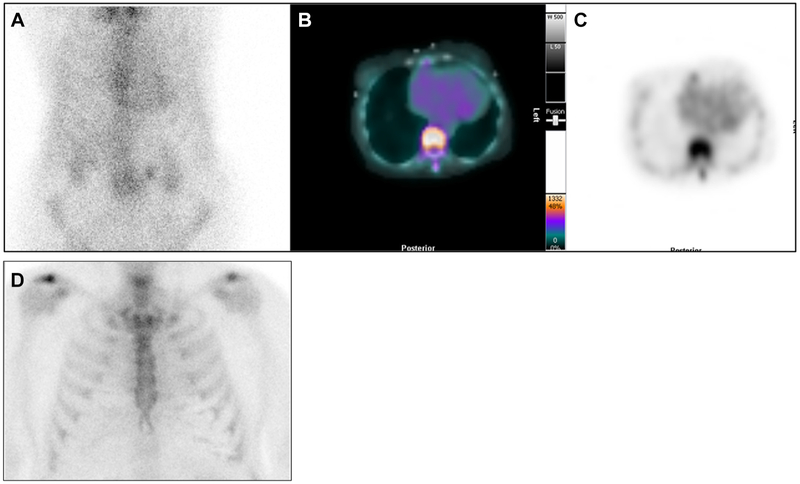
99mTc-PYP on the 1-hour planar chest images and corresponding cardiac SPECT images. 99mTc-PYP with Grade 2 cardiac uptake on the planar chest images (A), which was confirmed as blood pool activity on SPECT/CT fusion images (B), and SPECT images (C). These are 1-hour images, and low rib uptake is noted. In contrast, Panel D shows 3-hour planar chest images from another patient showing Grade 0 (no) cardiac uptake and expected rib uptake.
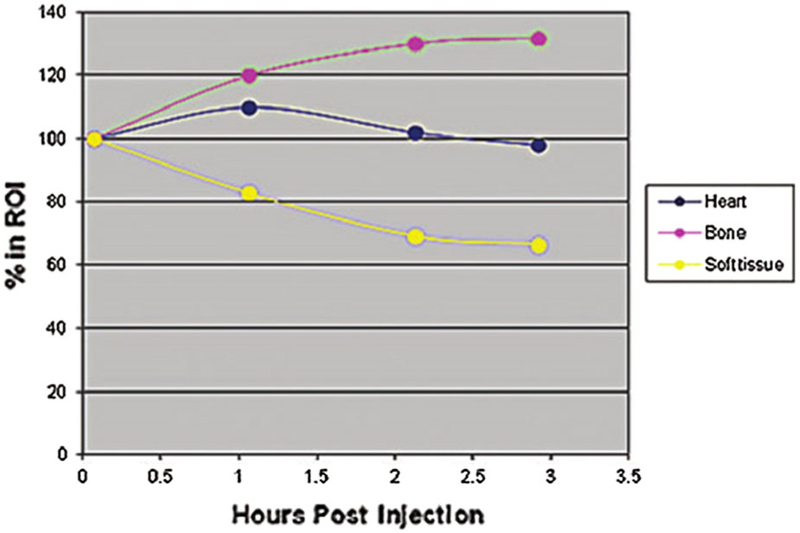
Changes in heart and bone 99mTc-DPD counts over time. Hutt et al. evaluated planar images at multiple time points after injection of 99mTc-DPD in 4 patients. As seen in this figure, myocardial counts peaked at 60 minutes, while bone counts peaked between 2 and 3 hours after injection of 99mTc-DPD.
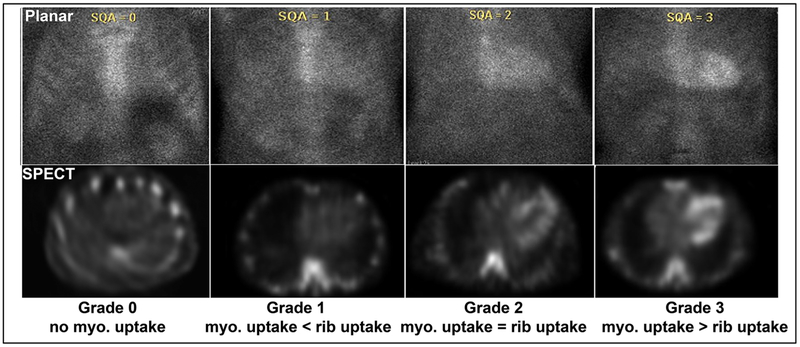
Visual grading of 99mTc PYP planar and SPECT scans. 99mTc pyrophosphate (PYP) scans are graded visually into Grades 0, 1, 2, and 3, comparing myocardial radiotracer uptake-to-rib uptake. Myo = myocardial. Grades 2 and 3 are considered positive for ATTR cardiac amyloidosis. Figure reproduced with permission.
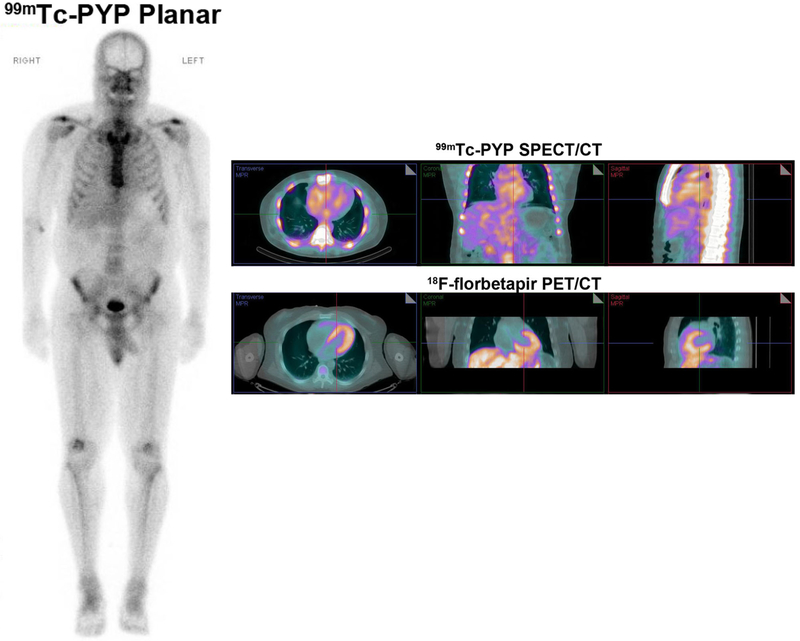
A negative 99mTc-pyrophosphate scan does not exclude cardiac amyloidosis. A 59-year-old man with Val 122 I mutation and heart failure had typical echocardiographic findings. He was referred for 99mTc-PYP imaging which was negative (Grade 0 uptake on planar whole-body images on the left; SPECT/CT fusion images in the right panel, top row show blood pool activity without myocardial uptake). Further evaluation with serum and urine immunofixation, and bone marrow biopsy confirmed AL amyloidosis. A PET/CT scan obtained as part of a research protocol using 8 mCi 18F-florbetapir with dynamic imaging, and static images reconstructed from 4 to 30 minutes, showed intense myocardial uptake (PET/CT fusion images on the right panel bottom row) confirming cardiac amyloidosis.
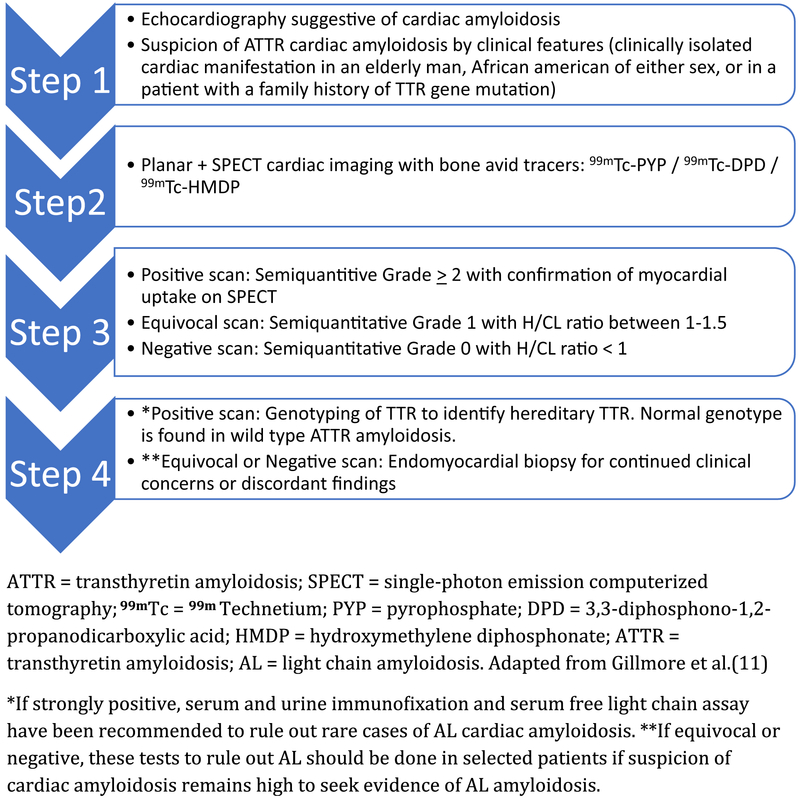
A proposed algorithm incorporating 99mTc-PYP, DPD, and HMDP for the evaluation of suspected ATTR cardiac amyloidosis. Evaluation of patients with suspected cardiac amyloidosis typically starts with echocardiography or CMR to evaluate cardiac structure and function, and if ATTR is suspected a bone avid scintigraphy is performed. If the bone avid tracer cardiac scintigraphy is strongly positive, and monoclonal protein is excluded, transthyretin cardiac amyloidosis is diagnosed with higher specificity. In equivocal or negative cases, further evaluation may be considered including endomyocardial biopsy.
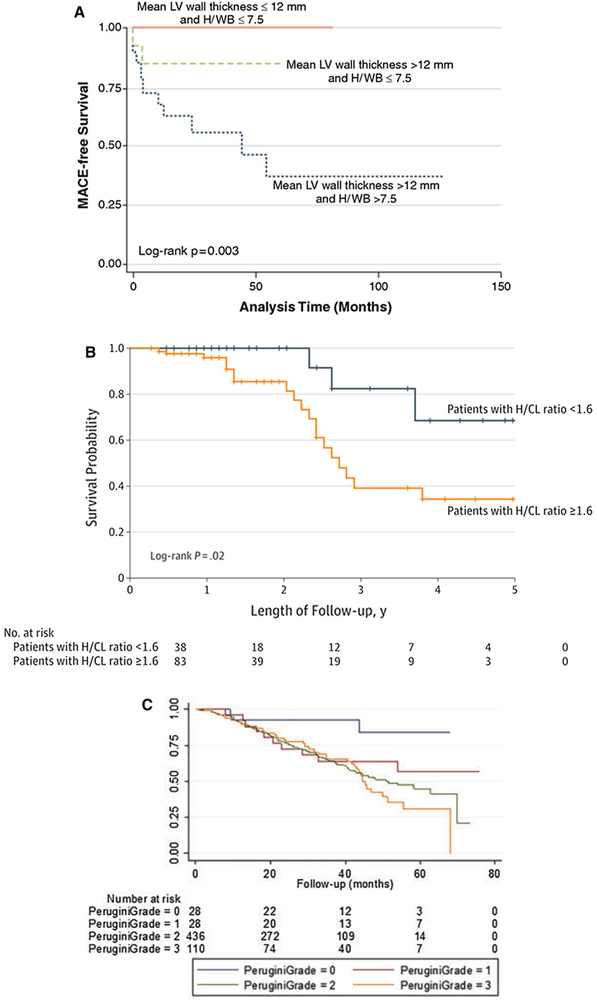
Prognostic value of 99mTc-DPD/PYP imaging in cardiac amyloidosis. Patients with mean LV wall thickness < 12 mm, heart-to-whole body retention (H/WB) ratio < 7.5 on 99mTc-DPD (A), heart/contralateral (H/CL) ratio < 1.6 on 99mTc-PYP (B), and Grade 0 uptake on 99mTc-DPD (C) showed best outcomes. Patients with Perugini Grades 1, 2, and 3 showed similar survival, and worse compared to Grades 0 (no amyloidosis). Figures reproduced with permission from refs. ,,
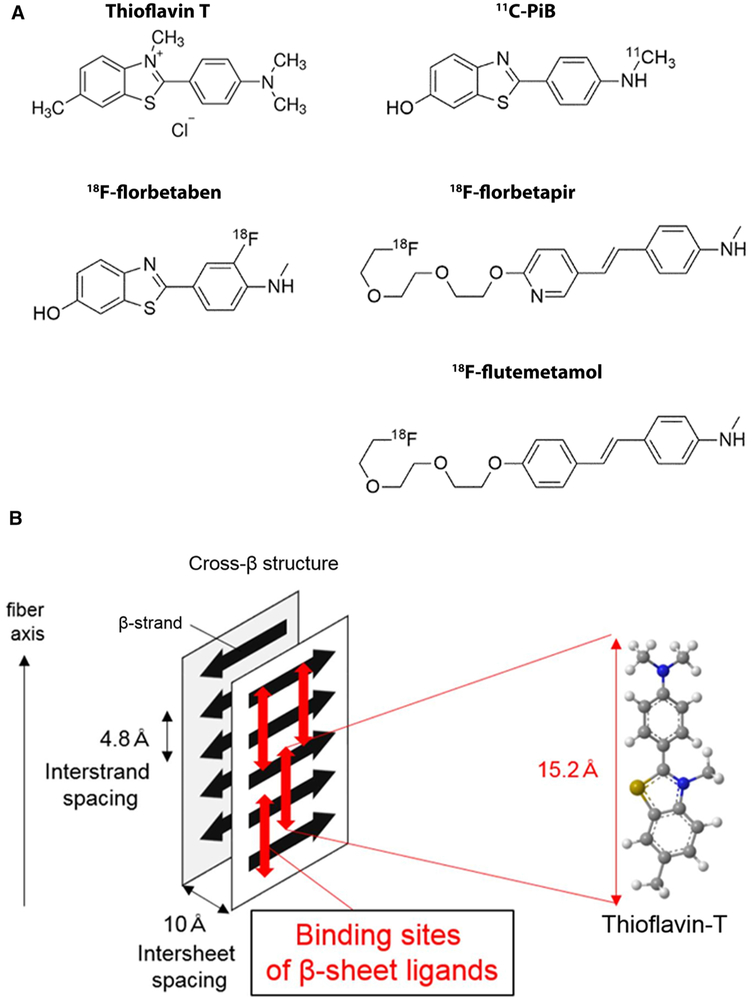
Amyloid PET tracers (A) and proposed mechanism of binding of amyloid PET radiotracers (B). 18F-florbetapir, 18F-florbetaben, and 18F-flutemetamol are FDA approved for β-amyloid imaging in Alzheimer’s disease. 11C-PIB is not FDA approved. Studies have reported the utility of the 11C-PIB, 18F-florbetapir, and 18F-florbetaben for imaging AL and ATTR cardiac amyloidosis, and these tracers appear to show greater uptake in AL than ATTR cardiac amyloidosis. These tracers are structurally similar to Thioflavin T and likely bind to the motif of the β pleated sheet structure. Molecular structures in Figure 10A were adapted from package inserts/product catalogue and reproduced with permission from ref.
Figure 10B reproduced with permission from ref.
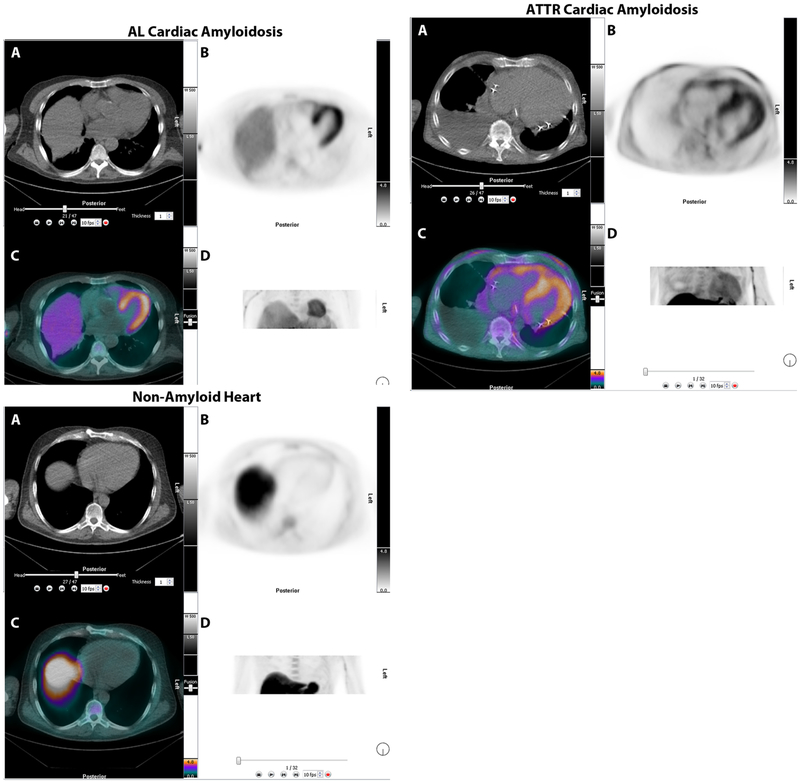
18F-florbetapir PET/CT imaging in patients with AL, ATTR, and no-amyloidosis. Images are displayed as axial CT transmission (A), axial emission (B), fused transmission/emission (C), and a maximum intensity projection image (D). Both AL (top left), ATTR (top right) images show intense 18F-florbetapir uptake in the left ventricle. The patient without amyloidosis, volunteer, (bottom), showed no myocardial uptake of 18F-florbetapir.
References
-
- Adams D, Gonzalez-Duarte A, O’Riordan WD, Yang CC, Ueda M, Adams AV, et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. N Engl J Med 2018;379:11–21. - PubMed
-
- Benson MD, Waddington-Cruz M, Berk JL, Polydefkis M, Dyck PJ, Wang AK, et al. Inotersen Treatment for Patients with Hereditary Transthyretin Amyloidosis. N Engl J Med 2018;379:22–31. - PubMed
-
- Falk RH. Diagnosis and management of the cardiac amyloidoses. Circulation 2005;112:2047–60. - PubMed
-
- Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol 1995;32:45–59. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
