

Safely Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge
- PMID: 30571347
- PMCID: PMC6309794
- DOI: 10.1161/CIRCULATIONAHA.118.036528
Safely Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge
Abstract
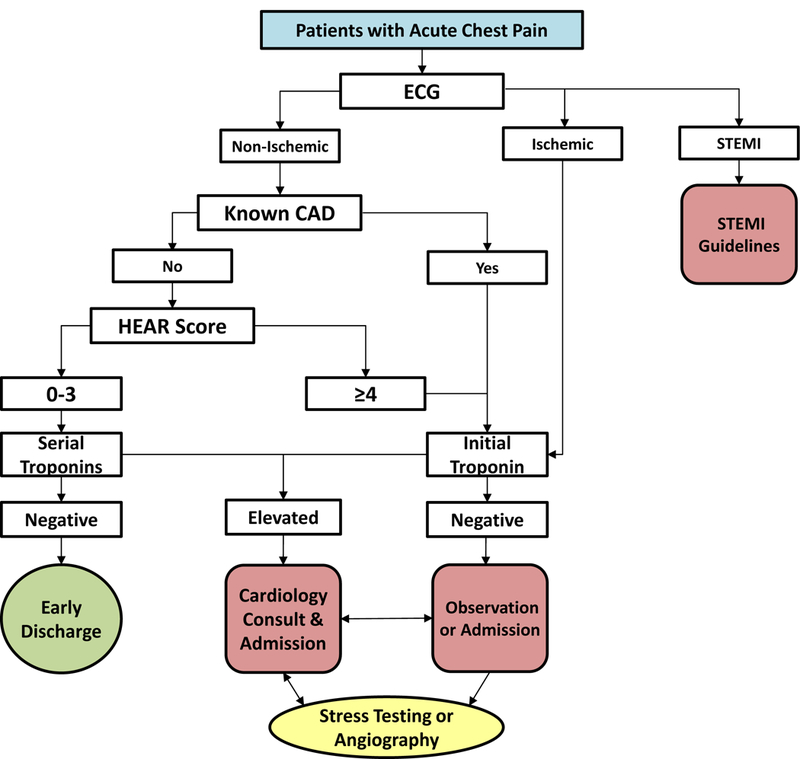
Background: The HEART Pathway (history, ECG, age, risk factors, and initial troponin) is an accelerated diagnostic protocol designed to identify low-risk emergency department patients with chest pain for early discharge without stress testing or angiography. The objective of this study was to determine whether implementation of the HEART Pathway is safe (30-day death and myocardial infarction rate <1% in low-risk patients) and effective (reduces 30-day hospitalizations) in emergency department patients with possible acute coronary syndrome.
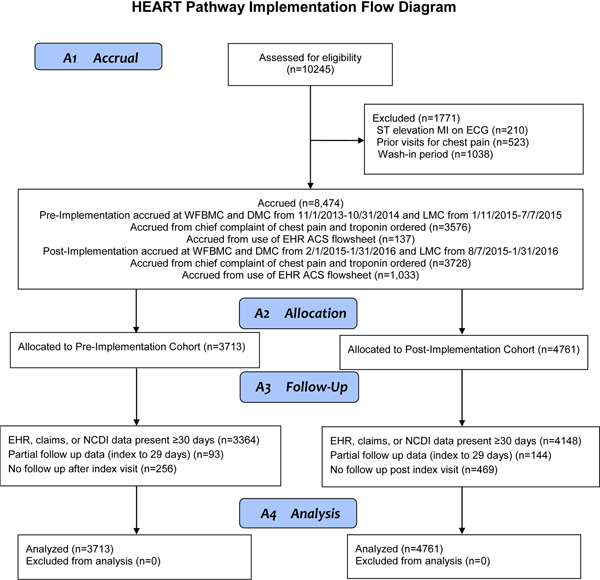
Methods: A prospective pre-post study was conducted at 3 US sites among 8474 adult emergency department patients with possible acute coronary syndrome. Patients included were ≥21 years old, investigated for possible acute coronary syndrome, and had no evidence of ST-segment-elevation myocardial infarction on ECG. Accrual occurred for 12 months before and after HEART Pathway implementation from November 2013 to January 2016. The HEART Pathway accelerated diagnostic protocol was integrated into the electronic health record at each site as an interactive clinical decision support tool. After accelerated diagnostic protocol integration, ED providers prospectively used the HEART Pathway to identify patients with possible acute coronary syndrome as low risk (appropriate for early discharge without stress testing or angiography) or non-low risk (appropriate for further in-hospital evaluation). The primary safety and effectiveness outcomes, death, and myocardial infarction (MI) and hospitalization rates at 30 days were determined from health records, insurance claims, and death index data.
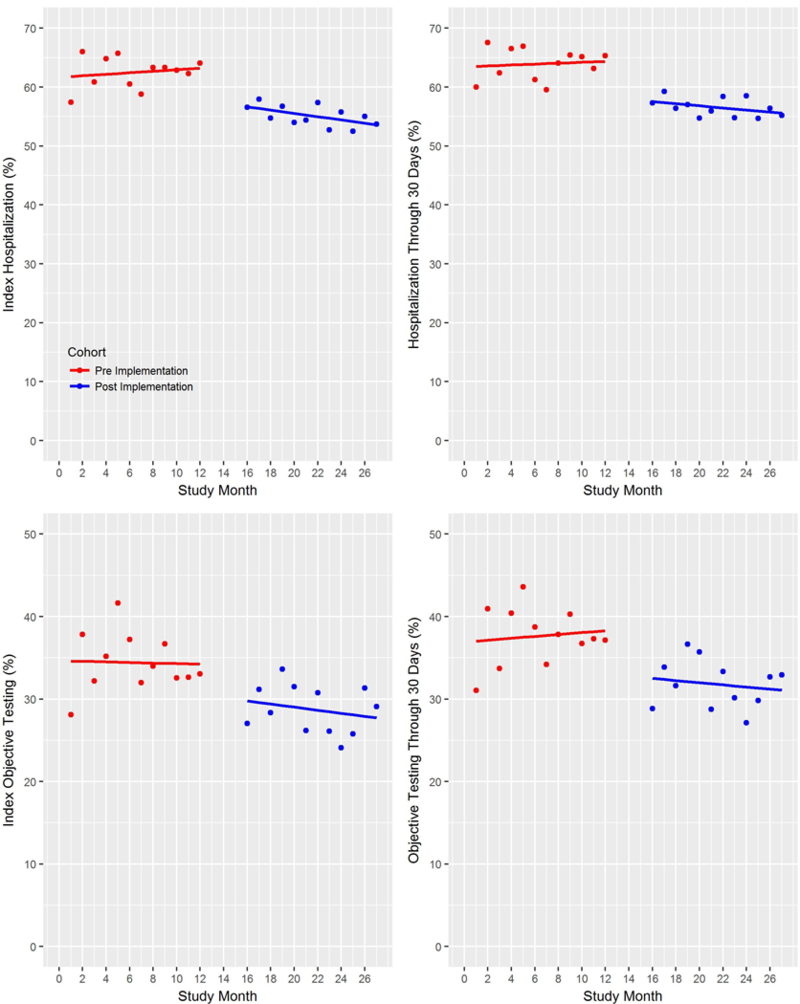
Results: Preimplementation and postimplementation cohorts included 3713 and 4761 patients, respectively. The HEART Pathway identified 30.7% as low risk; 0.4% of these patients experienced death or MI within 30 days. Hospitalization at 30 days was reduced by 6% in the postimplementation versus preimplementation cohort (55.6% versus 61.6%; adjusted odds ratio, 0.79; 95% CI, 0.71-0.87). During the index visit, more MIs were detected in the postimplementation cohort (6.6% versus 5.7%; adjusted odds ratio, 1.36; 95% CI, 1.12-1.65). Rates of death or MI during follow-up were similar (1.1% versus 1.3%; adjusted odds ratio, 0.88; 95% CI, 0.58-1.33).
Conclusions: HEART Pathway implementation was associated with decreased hospitalizations, increased identification of index visit MIs, and a very low death and MI rate among low-risk patients. These findings support use of the HEART Pathway to identify low-risk patients who can be safely discharged without stress testing or angiography.
Clinical trial registration: URL: http://www.clinicaltrials.gov . Unique identifier: NCT02056964.
Keywords: acute coronary syndrome; clinical decision making; decision support systems, clinical; electronic health records; emergency medicine; risk assessment.
Figures
Comment in
-
Response by Mahler et al to Letter Regarding Article, "Safely Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge: HEART Pathway Accelerated Diagnostic Protocol".Circulation. 2019 May 7;139(19):e915-e916. doi: 10.1161/CIRCULATIONAHA.119.039922. Circulation. 2019. PMID: 31059320 No abstract available.
-
Letter by Hafner et al Regarding Article, "Safely Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge: HEART Pathway Accelerated Diagnostic Protocol".Circulation. 2019 May 7;139(19):e913-e914. doi: 10.1161/CIRCULATIONAHA.119.039615. Circulation. 2019. PMID: 31059322 No abstract available.
References
-
- Owens PL, Barrett ML, Gibson TB, Andrews RM, Weinick RM, Mutter RL. Emergency department care in the united states: A profile of national data sources. Ann Emerg Med. 2010;56:150–165. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, Griffith JL, Selker HP. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342:1163–1170. - PubMed
-
- Pines JM, Isserman JA, Szyld D, Dean AJ, McCusker CM, Hollander JE. The effect of physician risk tolerance and the presence of an observation unit on decision making for ed patients with chest pain. Am J Emerg Med. 2010;28:771–779. - PubMed
-
- Fleischmann KE, Goldman L, Johnson PA, Krasuski RA, Bohan JS, Hartley LH, Lee TH. Critical pathways for patients with acute chest pain at low risk. J Thromb Thrombolysis. 2002;13:89–96. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit JA, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Rosamond WD, Sorlie PD, Stafford RS, Turan TN, Turner MB, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics−−2011 update: A report from the american heart association. Circulation. 2011;123:e18–e209. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
