

Association Between Driving Distance From Nearest Fire Station and Survival of Out-of-Hospital Cardiac Arrest
- PMID: 30571383
- PMCID: PMC6404193
- DOI: 10.1161/JAHA.118.008771
Association Between Driving Distance From Nearest Fire Station and Survival of Out-of-Hospital Cardiac Arrest
Abstract
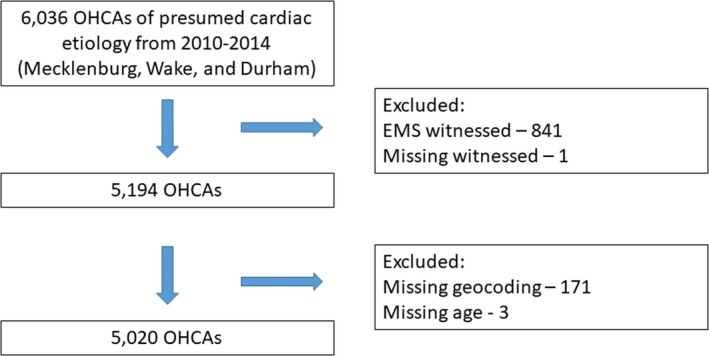
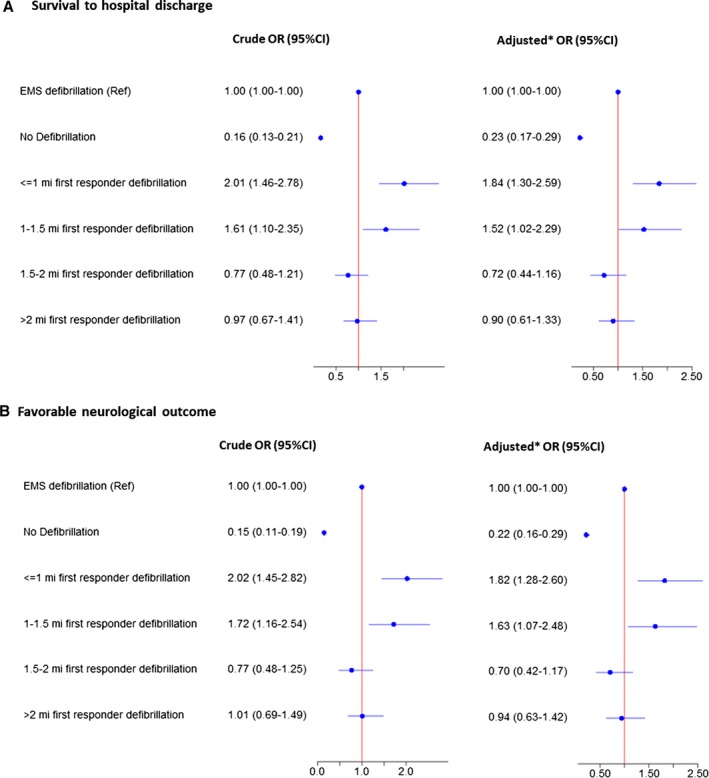
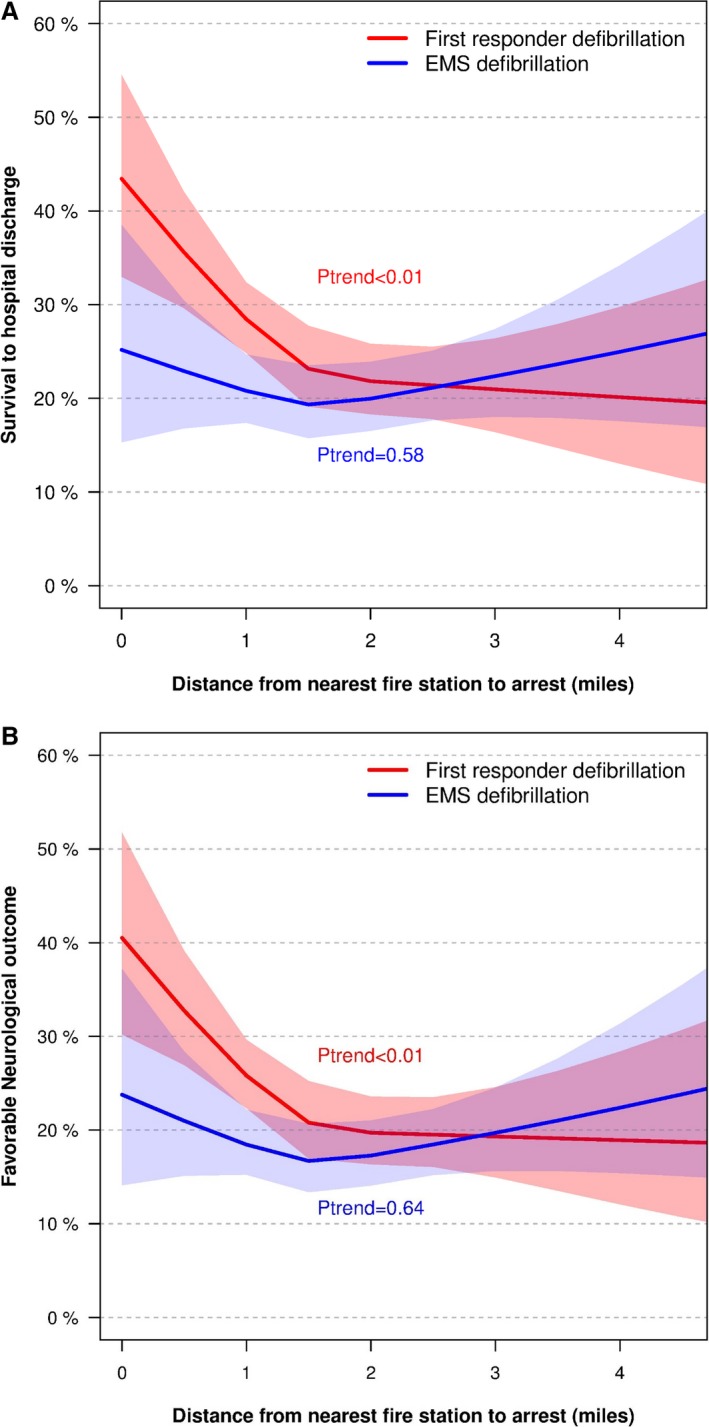
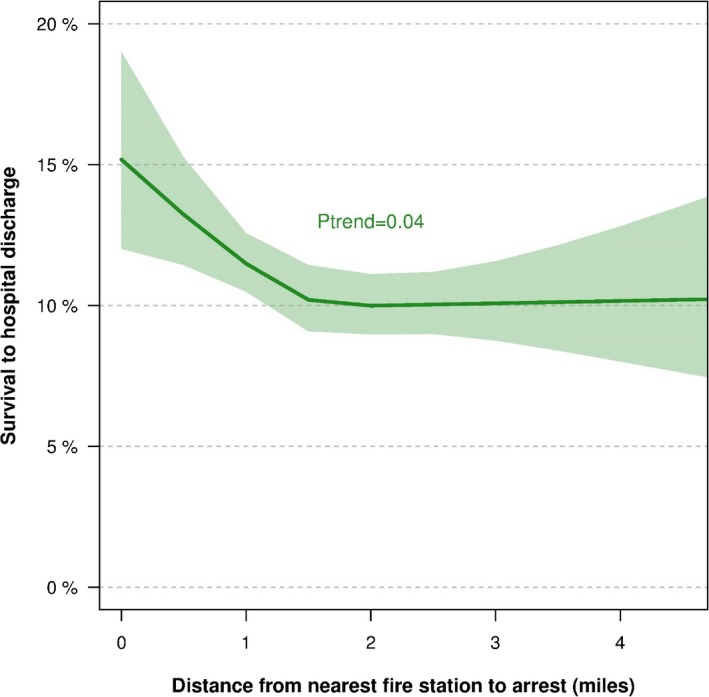
Background Firefighter first responders dispatched in parallel with emergency medical services ( EMS ) personnel for out-of-hospital cardiac arrests ( OHCA ) can provide early defibrillation to improve survival. We examined whether survival following first responder defibrillation differed according to driving distance from nearest fire station to OHCA site. Methods and Results From the CARES (Cardiac Arrest Registry to Enhance Survival) registry, we identified non- EMS witnessed OHCA s of presumed cardiac cause from 2010 to 2014 in Durham, Mecklenburg, and Wake counties, North Carolina. We used logistic regression to estimate the association between calculated driving distances (≤1, 1-1.5, 1.5-2, and >2 miles) and survival to hospital discharge following first responder defibrillation compared with defibrillation by EMS personnel. In total, 5020 OHCA s were included in the study. First responders more often applied the first automated external defibrillators at the shortest distances (≤1 mile) versus longest distances (>2 miles) (53.4% versus 46.6%, respectively, P<0.001). When compared with EMS defibrillation, first responder defibrillation within 1 mile and 1 to 1.5 miles of the nearest fire station was associated with increased survival to hospital discharge (odds ratio 2.01 [95% confidence interval 1.46-2.78] and odds ratio 1.61 [95% confidence interval 1.10-2.35], respectively). However, at the longest distances (1.5-2.0 and >2.0 miles), survival following first responder defibrillation did not differ from EMS defibrillation (odds ratio 0.77 [95% confidence interval 0.48-1.21] and odds ratio 0.97 [95% confidence interval 0.67-1.41], respectively). Conclusions Shorter driving distance from nearest fire station to OHCA location was associated with improved survival following defibrillation by first responders. These results suggest that the location of first responder units should be considered when organizing prehospital systems of OHCA care.
Keywords: driving distance; early defibrillation; firefighter; first responder; out‐of‐hospital cardiac arrest.
Figures
References
-
- Caffrey SL, Willoughby PJ, Pepe PE, Becker LB. Public use of automated external defibrillators. N Engl J Med. 2002;347:1242–1247. - PubMed
-
- Page RL, Joglar JA, Kowal RC, Zagrodzky JD, Nelson LL, Ramaswamy K, Barbera SJ, Hamdan MH, McKenas DK. Use of automated external defibrillators by a U.S. airline. N Engl J Med. 2000;343:1210–1216. - PubMed
-
- Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343:1206–1209. - PubMed
-
- Renkiewicz GK, Hubble MW, Wesley DR, Dorian PA, Losh MJ, Swain R, Taylor SE. Probability of a shockable presenting rhythm as a function of EMS response time. Prehosp Emerg Care. 2014;18:224–230. - PubMed
-
- Waalewijn RA, Nijpels MA, Tijssen JG, Koster RW. Prevention of deterioration of ventricular fibrillation by basic life support during out‐of‐hospital cardiac arrest. Resuscitation. 2002;54:31–36. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
