

Ambulatory assessment of phonotraumatic vocal hyperfunction using glottal airflow measures estimated from neck-surface acceleration
- PMID: 30571719
- PMCID: PMC6301575
- DOI: 10.1371/journal.pone.0209017
Ambulatory assessment of phonotraumatic vocal hyperfunction using glottal airflow measures estimated from neck-surface acceleration
Abstract
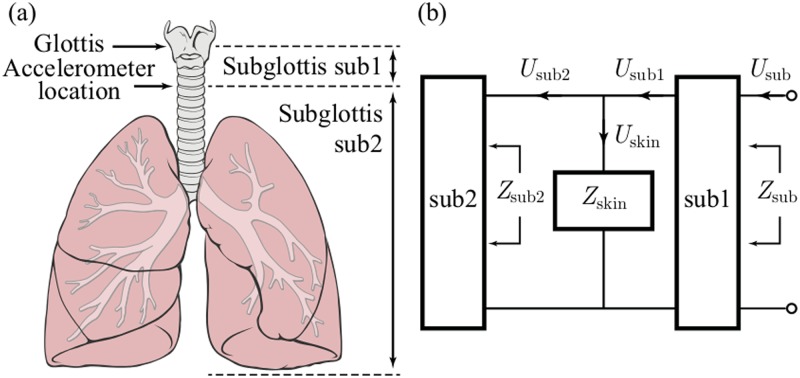
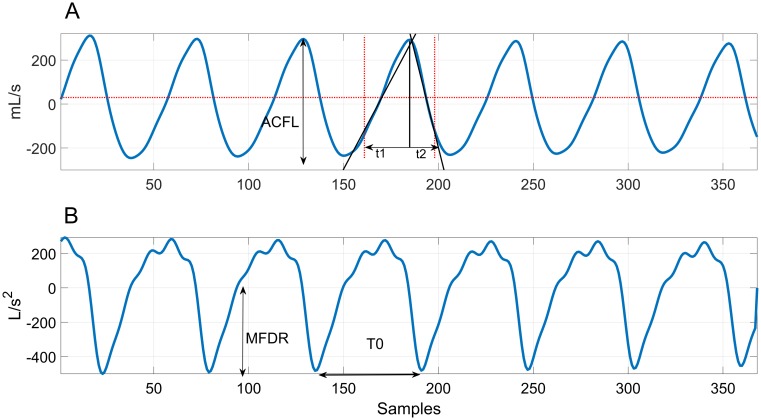
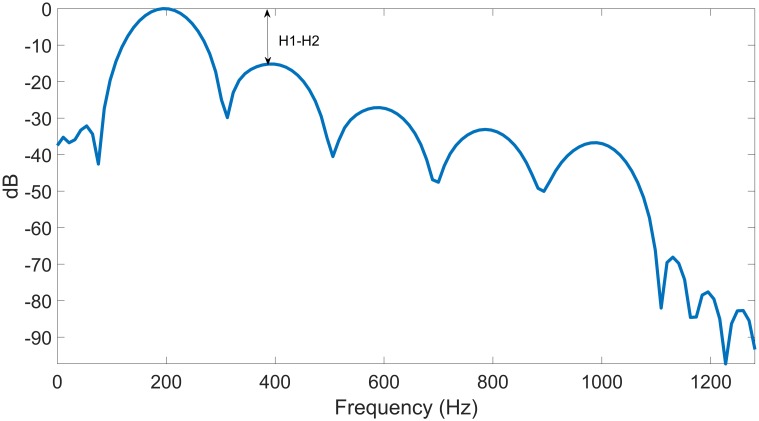
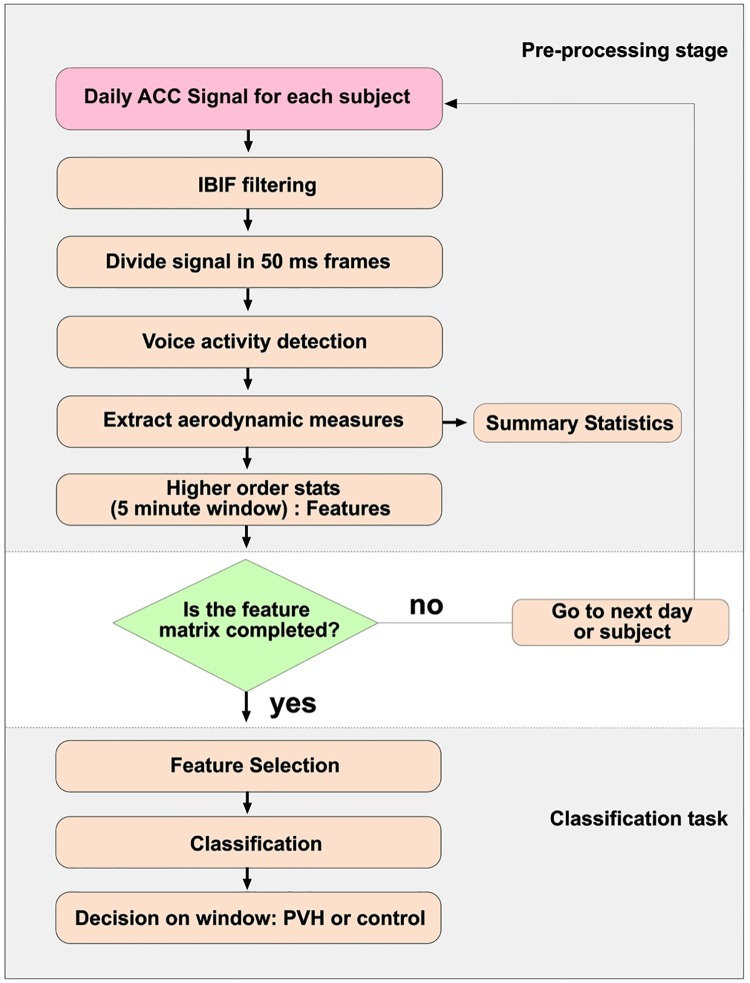
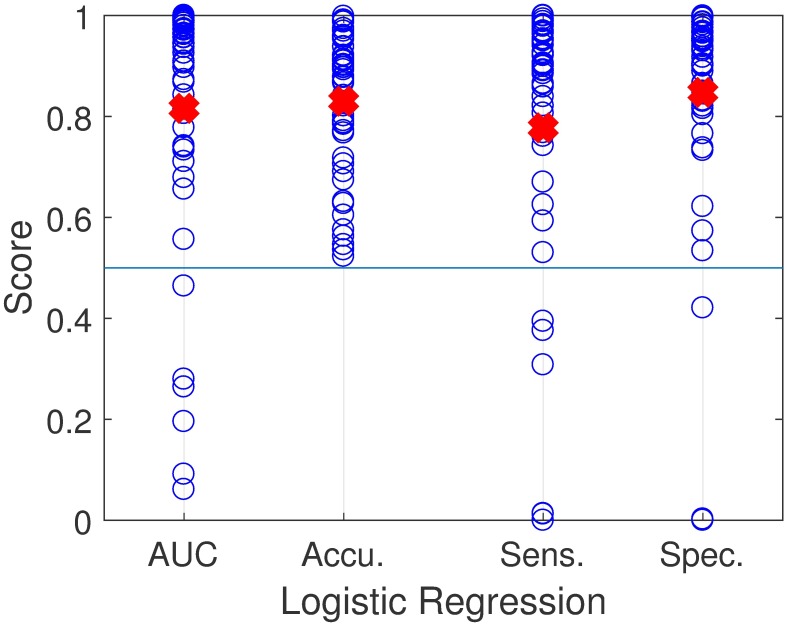
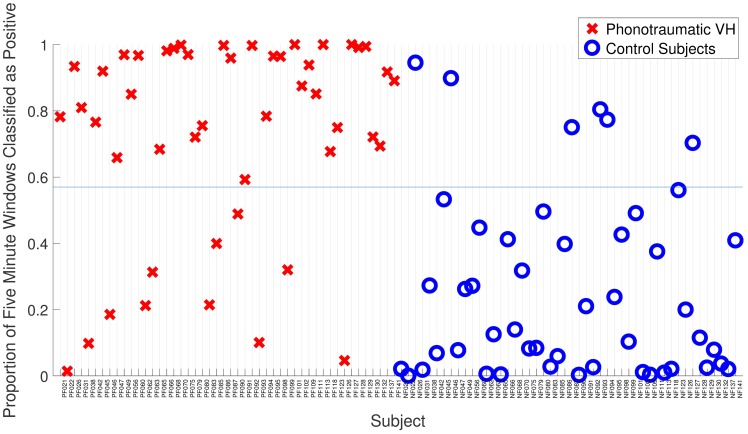
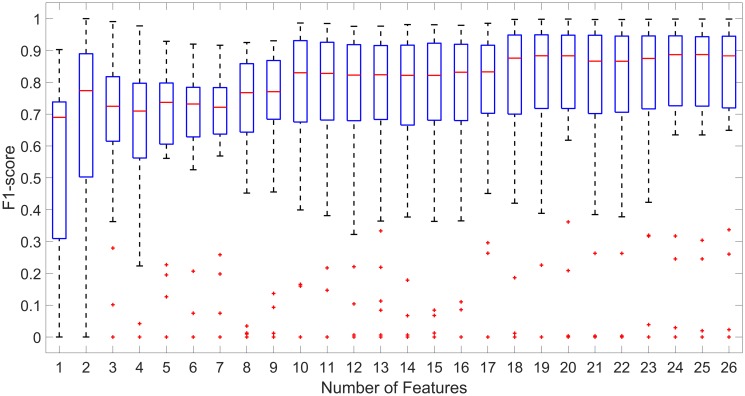
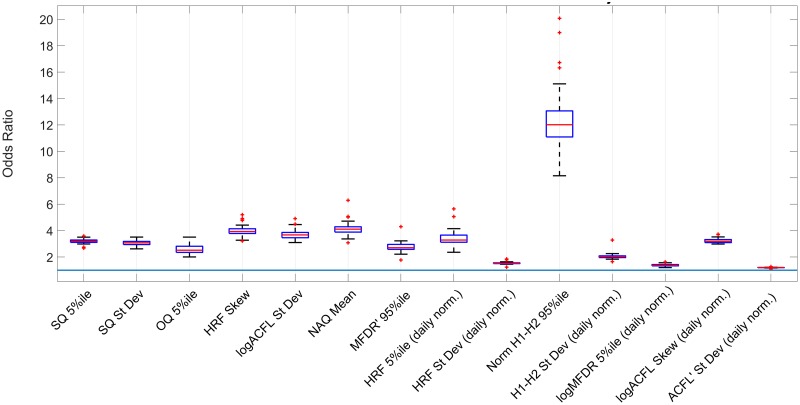
Phonotraumatic vocal hyperfunction (PVH) is associated with chronic misuse and/or abuse of voice that can result in lesions such as vocal fold nodules. The clinical aerodynamic assessment of vocal function has been recently shown to differentiate between patients with PVH and healthy controls to provide meaningful insight into pathophysiological mechanisms associated with these disorders. However, all current clinical assessment of PVH is incomplete because of its inability to objectively identify the type and extent of detrimental phonatory function that is associated with PVH during daily voice use. The current study sought to address this issue by incorporating, for the first time in a comprehensive ambulatory assessment, glottal airflow parameters estimated from a neck-mounted accelerometer and recorded to a smartphone-based voice monitor. We tested this approach on 48 patients with vocal fold nodules and 48 matched healthy-control subjects who each wore the voice monitor for a week. Seven glottal airflow features were estimated every 50 ms using an impedance-based inverse filtering scheme, and seven high-order summary statistics of each feature were computed every 5 minutes over voiced segments. Based on a univariate hypothesis testing, eight glottal airflow summary statistics were found to be statistically different between patient and healthy-control groups. L1-regularized logistic regression for a supervised classification task yielded a mean (standard deviation) area under the ROC curve of 0.82 (0.25) and an accuracy of 0.83 (0.14). These results outperform the state-of-the-art classification for the same classification task and provide a new avenue to improve the assessment and treatment of hyperfunctional voice disorders.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
