

Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on stunting and anaemia among HIV-exposed children in rural Zimbabwe: a cluster-randomised controlled trial
- PMID: 30573417
- PMCID: PMC6472652
- DOI: 10.1016/S2352-4642(18)30340-7
Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on stunting and anaemia among HIV-exposed children in rural Zimbabwe: a cluster-randomised controlled trial
Abstract
Background: Children exposed to HIV have a high prevalence of stunting and anaemia. We aimed to test the effect of improved infant and young child feeding (IYCF) and improved water, sanitation, and hygiene (WASH) on child linear growth and haemoglobin concentrations.
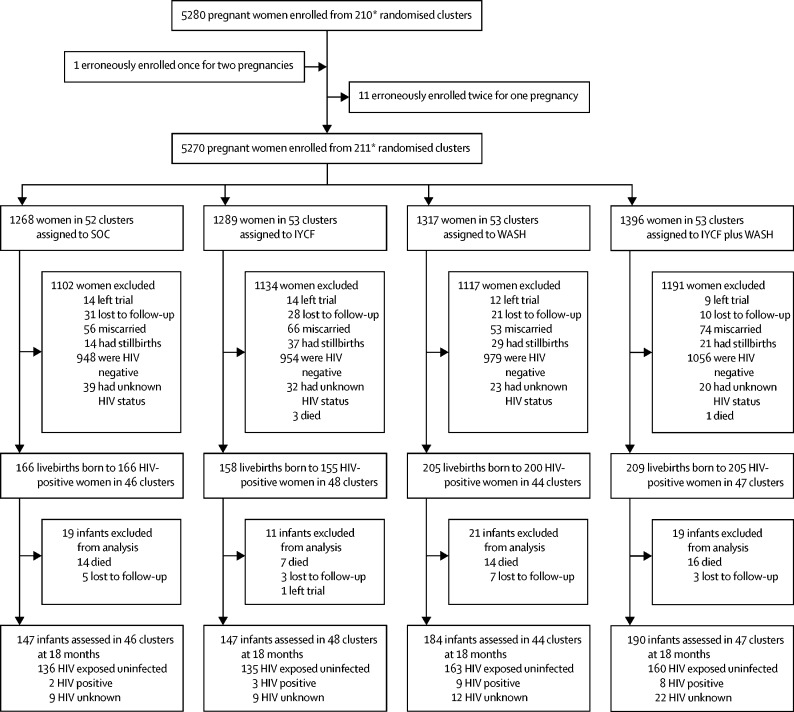
Methods: We did a cluster randomised 2 × 2 factorial trial in two districts in rural Zimbabwe. Women were eligible for inclusion if they permanently lived in the trial clusters (ie, the catchment area of between one and four village health workers employed by the Zimbabwean Ministry of Health and Child Care) and were confirmed pregnant. Clusters were randomly allocated to standard of care (52 clusters); IYCF (20 g small-quantity lipid-based nutrient supplement daily for infants from 6 months to 18 months, complementary feeding counselling with context-specific messages, longitudinal delivery, and reinforcement; 53 clusters); WASH (ventilated, improved pit latrine, two hand-washing stations, liquid soap, chlorine, play space, and hygiene counselling; 53 clusters); or IYCF plus WASH (53 clusters). Participants and fieldworkers were not masked. Our co-primary outcomes were length for age Z score and haemoglobin in infants at 18 months of age. Here, we report these outcomes in the HIV-exposed children, analysed by intention to treat. We estimated the effects of the interventions by comparing the two IYCF groups with the two non-IYCF groups and the two WASH groups with the two non-WASH groups, except for outcomes with an important statistical interaction between the interventions. The trial is registered at ClinicalTrials.gov (NCT01824940) and is now complete.
Findings: Between Nov 22, 2012, and March 27, 2015, 726 HIV-positive pregnant women were included in the trial. 668 children were evaluated at 18 months (147 from 46 standard of care clusters; 147 from 48 IYCF clusters; 184 from 44 WASH clusters; 190 from 47 IYCF plus WASH clusters). Of the 668 children, 22 (3%) were HIV-positive, 594 (89%) HIV-exposed uninfected, and 52 (8%) HIV-unknown. The IYCF intervention increased mean length for age Z score by 0·26 (95% CI 0·09-0·43; p=0·003) and haemoglobin concentration by 2·9 g/L (95% CI 0·90-4·90; p=0·005). 165 (50%) of 329 children in the non-IYCF groups were stunted, compared with 136 (40%) of 336 in the IYCF groups (absolute difference 10%, 95% CI 2-17); and the prevalence of anaemia was also lower in the IYCF groups (45 [14%] of 319) than in the non-IYCF groups (24 [7%] of 329; absolute difference 7%, 95% CI 2-12). The WASH intervention had no effect on length or haemoglobin concentration. There were no trial-related adverse or serious adverse events.
Interpretation: Since HIV-exposed children are particularly vulnerable to undernutrition and responded well to improved complementary feeding, IYCF interventions could have considerable benefits in areas of high antenatal HIV prevalence. However, elementary WASH interventions did not lead to improvements in growth.
Funding: Bill & Melinda Gates Foundation, UK Aid, Wellcome Trust, Swiss Development Cooperation, US National Institutes of Health, and UNICEF.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Similar articles
-
Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on child stunting and anaemia in rural Zimbabwe: a cluster-randomised trial.Lancet Glob Health. 2019 Jan;7(1):e132-e147. doi: 10.1016/S2214-109X(18)30374-7. Lancet Glob Health. 2019. PMID: 30554749 Free PMC article. Clinical Trial.
-
Independent and combined effects of improved water, sanitation, and hygiene (WASH) and improved complementary feeding on early neurodevelopment among children born to HIV-negative mothers in rural Zimbabwe: Substudy of a cluster-randomized trial.PLoS Med. 2019 Mar 21;16(3):e1002766. doi: 10.1371/journal.pmed.1002766. eCollection 2019 Mar. PLoS Med. 2019. PMID: 30897095 Free PMC article. Clinical Trial.
-
Effects of improved complementary feeding and improved water, sanitation and hygiene on early child development among HIV-exposed children: substudy of a cluster randomised trial in rural Zimbabwe.BMJ Glob Health. 2020 Jan 13;5(1):e001718. doi: 10.1136/bmjgh-2019-001718. eCollection 2020. BMJ Glob Health. 2020. PMID: 32133164 Free PMC article. Clinical Trial.
-
Summarizing the Child Growth and Diarrhea Findings of the Water, Sanitation, and Hygiene Benefits and Sanitation Hygiene Infant Nutrition Efficacy Trials.Nestle Nutr Inst Workshop Ser. 2020;93:153-166. doi: 10.1159/000503350. Epub 2020 Jan 28. Nestle Nutr Inst Workshop Ser. 2020. PMID: 31991427 Review.
-
Nutritional interventions for preventing stunting in children (birth to 59 months) living in urban slums in low- and middle-income countries (LMIC).Cochrane Database Syst Rev. 2019 Jun 17;6(6):CD011695. doi: 10.1002/14651858.CD011695.pub2. Cochrane Database Syst Rev. 2019. PMID: 31204795 Free PMC article.
Cited by
-
Citrulline and kynurenine to tryptophan ratio: potential EED (environmental enteric dysfunction) biomarkers in acute watery diarrhea among children in Bangladesh.Sci Rep. 2023 Jan 25;13(1):1416. doi: 10.1038/s41598-023-28114-0. Sci Rep. 2023. PMID: 36697429 Free PMC article.
-
Food Insecurity and Water Insecurity in Rural Zimbabwe: Development of Multidimensional Household Measures.Int J Environ Res Public Health. 2021 Jun 3;18(11):6020. doi: 10.3390/ijerph18116020. Int J Environ Res Public Health. 2021. PMID: 34205143 Free PMC article.
-
How to design a complex behaviour change intervention: experiences from a nutrition-sensitive agriculture trial in rural India.BMJ Glob Health. 2020 Jun;5(6):e002384. doi: 10.1136/bmjgh-2020-002384. BMJ Glob Health. 2020. PMID: 32513863 Free PMC article. Review.
-
The gut microbiome and early-life growth in a population with high prevalence of stunting.Nat Commun. 2023 Feb 14;14(1):654. doi: 10.1038/s41467-023-36135-6. Nat Commun. 2023. PMID: 36788215 Free PMC article.
-
Combination of conditional cash transfer program and environmental health interventions reduces child mortality: an ecological study of Brazilian municipalities.BMC Public Health. 2021 Mar 31;21(1):627. doi: 10.1186/s12889-021-10649-4. BMC Public Health. 2021. PMID: 33789623 Free PMC article.
References
-
- UNAIDS UNAIDS data 2017. 2017. http://www.unaids.org/en/resources/documents/2017/20170720_Data_book_2017 (accessed Dw8).
-
- Evans C, Jones CE, Prendergast AJ. HIV-exposed, uninfected infants: new global challenges in the era of paediatric HIV elimination. Lancet Infect Dis. 2016;16:e92–e107. - PubMed
-
- Black RE, Victora CG, Walker SP. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382:427–451. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
