

Review
doi: 10.3174/ajnr.A5888.
Epub 2018 Dec 20.
High-Grade Gliomas in Children with Neurofibromatosis Type 1: Literature Review and Illustrative Cases
Affiliations
- PMID: 30573459
- PMCID: PMC7028622
- DOI: 10.3174/ajnr.A5888
Item in Clipboard
Review
High-Grade Gliomas in Children with Neurofibromatosis Type 1: Literature Review and Illustrative Cases
AJNR Am J Neuroradiol.
2019 Feb.
Abstract
High-grade gliomas in patients with neurofibromatosis type 1 are rare and may therefore not be considered in the differential of brain lesions. Here, we describe 5 children with neurofibromatosis type 1; four of them developed various types of high-grade gliomas. The fifth patient had imaging features concerning for a high-grade lesion, but tissue diagnosis showed a low-grade glioma. The cases and literature summary provided here are to raise awareness for the occurrence of high-grade gliomas in children with neurofibromatosis type 1 and the limited ability of imaging features alone to predict a high-grade malignancy.
© 2019 by American Journal of Neuroradiology.
Figures
A 7-year-old boy with NF1 and a pathologic diagnosis of a midline, H3 K27M–mutant glioblastoma (patient 1). Axial T1 postcontrast at baseline (A) and after 6 weeks of follow-up (B). Baseline (A, arrow) smoothly marginated T1 hypointense mass is shown centered within the midbrain and tectal plate with mild central enhancement; 6 weeks later, the mass increased in size (B, arrow) with new peripheral enhancement. Imaging at baseline shows a high diffusion signal on DWI (C) and a low signal on ADC (D), suggestive of high cellularity.
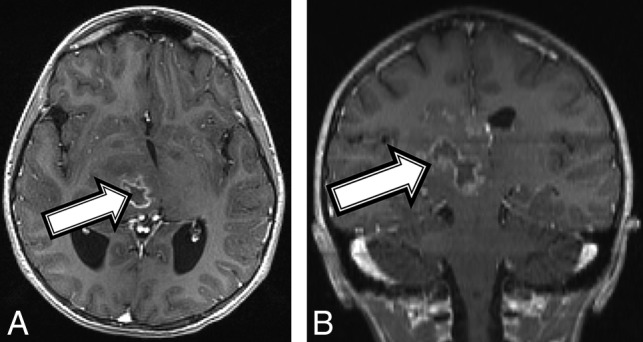
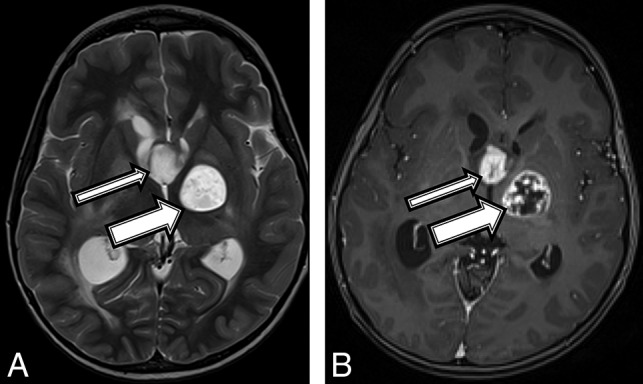
An 11-year-old girl with a final diagnosis of a grade II astrocytoma by histomorphology and a midline, diffuse HGG with H3 K27M mutation based on immunostaining (patient 2). Baseline axial T1 (A) and coronal (B) T1 postcontrast MR imaging shows a heterogeneous mass (A and B, arrows) centered in the right thalamus with a peripherally enhancing central cyst or area of necrosis.
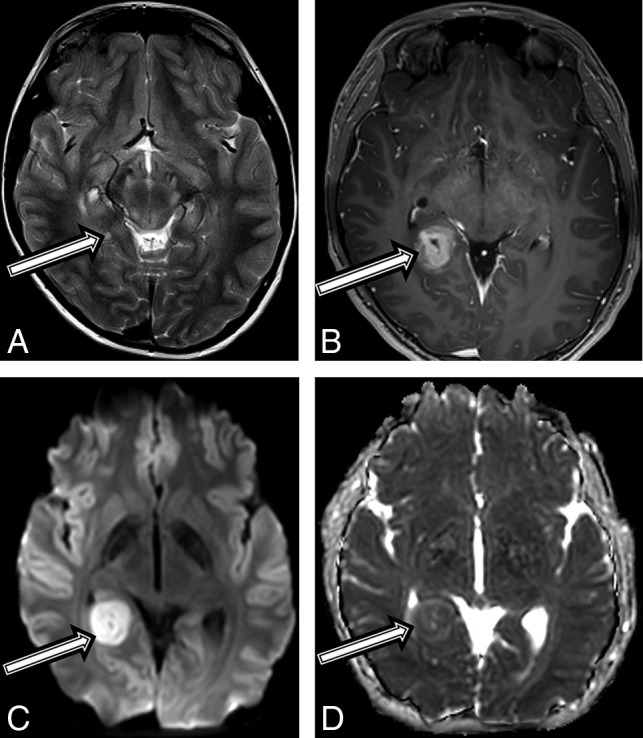
A 10-year-old boy with a final diagnosis of an anaplastic pleomorphic xanthoastrocytoma (patient 3). Axial T2-weighted images at baseline (A) and postcontrast axial T1 at 21 months (B) after diagnosis show a growing, well-defined mass in the right posterior mesial temporal lobe (A, arrow), which developed new inhomogeneous enhancement (B, arrow). MR imaging at 21 months shows new high-diffusion signal on DWI (C) and low signal on ADC (D), suggestive of high cellularity.
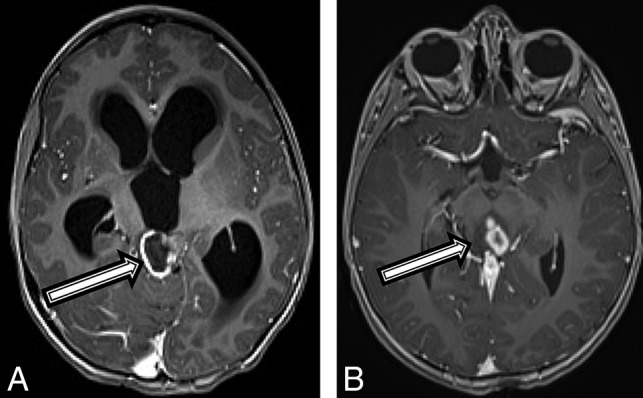
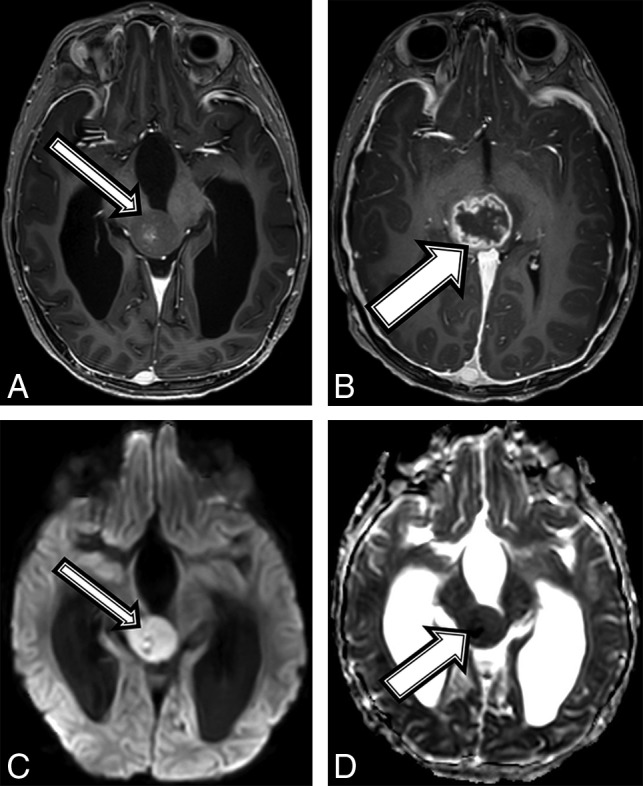
A 4-year-old boy with a diffuse HGG with H3 K27M mutation (patient 4). Axial T1 postcontrast MR imaging (A) at the initial presentation and on 6-month follow-up (B). There was initially a peripherally enhancing T2 hyperintense mass centered within the tectum (A, arrow) causing hydrocephalus. After 6 months, the lesion has increased in size, peripheral enhancement is no longer seen, but multiple centrally enhancing lesions are seen (B, arrow).
A 7-year-old boy with a final diagnosis of a pilocytic astrocytoma (patient 5). Axial T2 (A) and T1 postcontrast (B) MR images demonstrate a robustly enhancing T2 hyperintense suprasellar mass (thin arrows) and a T1 hypointense, T2 hyperintense mass centered within the left globus pallidus (thick arrows) with robust peripheral and patchy central enhancement.
Comment in
-
Reply.AJNR Am J Neuroradiol. 2019 Jun;40(6):E32. doi: 10.3174/ajnr.A6062. Epub 2019 May 9. AJNR Am J Neuroradiol. 2019. PMID: 31072977 Free PMC article. No abstract available.
-
Patients with High-Grade Gliomas and Café-au-Lait Macules: Is Neurofibromatosis Type 1 the Only Diagnosis?AJNR Am J Neuroradiol. 2019 Jun;40(6):E30-E31. doi: 10.3174/ajnr.A6058. Epub 2019 May 9. AJNR Am J Neuroradiol. 2019. PMID: 31072978 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials